Compliance Just Got Easier: Stay ahead of regulatory changes with instant notifications on updates that matter.
['Bloodborne Pathogens']
['Bloodborne Pathogens']
2025-09-05T05:00:00Z
JOIN TODAY TO CONTINUE READING THIS ARTICLE & OTHER INDUSTRY NEWS!
You'll also get exclusive access to:
A database of easy-to-understand regulationsAsk unlimited questions to our expertsPre-led discussions forumsAnd more
TRY IT FREE TODAY
Already have an account? Log in now.

Copyright 2026 J. J. Keller & Associate, Inc. For re-use options please contact copyright@jjkeller.com or call 800-558-5011.
NewsIndustry NewsBloodborne PathogensSafety & HealthIn-Depth ArticleGeneral Industry SafetyBloodborne PathogensEnglishFocus AreaUSA
Unmasking the top three OSHA violations for bloodborne pathogens
2025-09-05T05:00:00Z
OSHA’s Bloodborne Pathogens standard at 29 CFR 1910.1030 has been around for decades, but it remains a source of confusion for employers. In fact, OSHA cited the standard almost 3,000 times in the last two fiscal years, making it a frequently violated standard in Part 1910.
Who’s covered?
If you have employees with occupational exposure, you have obligations under the standard. “Occupational exposure” refers to reasonably anticipated contact with blood or other potentially infectious materials (OPIM) that may result from the performance of an employee’s duties.
While most employers mistakenly associate bloodborne pathogens with “just” healthcare, you don’t have to be in the healthcare industry to come under the standard. For example, first-aid team members, custodians and maintenance workers, housekeeping and laundry personnel, laboratory technicians, correctional and law enforcement officers, and others may have occupational exposure too. It’s the employer's responsibility to determine which job classifications or specific tasks and procedures involve reasonably anticipated contact with blood or OPIM.
Which requirements trip employers up the most?
Once you figure out that you have employees with occupational exposure and that 1910.1030 applies, it may be helpful to know where your peers go wrong. It turns out the top three trouble spots for 1910.1030 violators in fiscal years 2023 and 2024 were:
- Paragraph (c) — Exposure control plan and exposure determination,
- Subparagraph (g)(2) — Information and training, and
- Paragraph (f) — Hepatitis B vaccination and post-exposure evaluation and follow-up.
We cover these three in more detail below; however, note that recordkeeping and compliance methods at 1910.1030(h) and (d), respectively, rounded out the top five violative paragraphs under the standard.
#1 Violation: Failure to develop and maintain an exposure control plan, including an exposure determination, 1910.1030(c)
OSHA requires a written plan to eliminate or minimize employee exposure. Covered employers must include:
- An exposure determination per 1910.1030(c)(2);
- A schedule and method of implementing paragraphs (d), (f), (g), and (h) of 1910.1030; and
- A procedure to evaluate circumstances surrounding exposure incidents.
The plan must be reviewed annually and as necessary to reflect changes in tasks, procedures, and positions that affect occupational exposure, as well as technological changes that eliminate or reduce occupational exposure. Annually, employers also must document in the plan that they have:
- Considered and begun using appropriate, commercially-available, effective safer medical devices designed to eliminate or minimize occupational exposure; and
- Solicited input from front-line employees in identifying, evaluating, and selecting effective engineering and work practice controls.
#2 Violation: Failure to provide effective information and training, 1910.1030(g)(2)
Employers must ensure that their employees with occupational exposure receive initial training that covers all elements in paragraph (g)(2) of the standard. This is prior to being placed in positions where occupational exposure may occur. Training must also be offered at least annually thereafter, and when new or modified tasks or procedures affect an employee’s occupational exposure.
However, HIV and HBV laboratory and production facility employees must receive specialized initial training, in addition to the training provided to all employees with occupational exposure.
It’s important (and required) that training be presented at an educational level and in a language that employees understand and that employees have the opportunity to ask the trainer questions. A trainer knowledgeable in the training elements as they relate to the workplace is mandated as well.
#3 Violation: Failure to offer hepatitis B vaccination and post-exposure evaluation and follow-up, 1910.1030(f)
Employers must offer the hepatitis B vaccine to employees with occupational exposure after the employees have received training and within 10 days of initial assignment to a job with occupational exposure. Employees who decline to accept the vaccination must sign the statement in 1910.1030 Appendix A.
If an occupationally exposed employee suffers an exposure incident, then post-exposure evaluation and follow-up must be made available. An “exposure incident” is a specific eye, mouth, other mucous membrane, non-intact skin, or parenteral contact with blood or OPIM. The evaluation and follow-up must be at no cost to the employee and include:
- Documenting the route(s) of exposure and the circumstances under which the exposure incident occurred;
- Identifying and testing the source individual for HBV and HIV infectivity, if the source individual consents or the law doesn’t require consent;
- Collecting and testing the exposed employee’s blood, if the employee consents;
- Offering post-exposure prophylaxis;
- Offering counseling; and
- Evaluating reported illnesses.
After evaluating the employee, the healthcare professional will provide a limited written opinion to the employer, but it will not offer any medical findings or diagnoses.
Key to remember: If you have employees with occupational exposure, you’re covered by the Bloodborne Pathogens standard and must comply with all the requirements outlined in 1910.1030. The top three trouble spots for violators in fiscal years 2023 and 2024 involved the written plan, employee training, and vaccination/evaluation.

NewsIndustry NewsBloodborne PathogensSafety & HealthIn-Depth ArticleGeneral Industry SafetyBloodborne PathogensEnglishFocus AreaUSA
Unmasking the top three OSHA violations for bloodborne pathogens
2025-09-05T05:00:00Z
Written by
rache_krubsack
Compliance Expert - EHS
rache_krubsack
OSHA 30-hour General Industry Safety and Health, 2023
M.L.I.S. (Master of Library and Information Science), University of Wisconsin-Milwaukee; B.A., Loras College
Compliance Expert at J. J. Keller & Associates specializing in HazCom, OSHA training requirements, and more. Rachel develops content and provides impactful news and regulatory insights.
OSHA’s Bloodborne Pathogens standard at 29 CFR 1910.1030 has been around for decades, but it remains a source of confusion for employers. In fact, OSHA cited the standard almost 3,000 times in the last two fiscal years, making it a frequently violated standard in Part 1910.
Who’s covered?
If you have employees with occupational exposure, you have obligations under the standard. “Occupational exposure” refers to reasonably anticipated contact with blood or other potentially infectious materials (OPIM) that may result from the performance of an employee’s duties.
While most employers mistakenly associate bloodborne pathogens with “just” healthcare, you don’t have to be in the healthcare industry to come under the standard. For example, first-aid team members, custodians and maintenance workers, housekeeping and laundry personnel, laboratory technicians, correctional and law enforcement officers, and others may have occupational exposure too. It’s the employer's responsibility to determine which job classifications or specific tasks and procedures involve reasonably anticipated contact with blood or OPIM.
Which requirements trip employers up the most?
Once you figure out that you have employees with occupational exposure and that 1910.1030 applies, it may be helpful to know where your peers go wrong. It turns out the top three trouble spots for 1910.1030 violators in fiscal years 2023 and 2024 were:
- Paragraph (c) — Exposure control plan and exposure determination,
- Subparagraph (g)(2) — Information and training, and
- Paragraph (f) — Hepatitis B vaccination and post-exposure evaluation and follow-up.
We cover these three in more detail below; however, note that recordkeeping and compliance methods at 1910.1030(h) and (d), respectively, rounded out the top five violative paragraphs under the standard.
#1 Violation: Failure to develop and maintain an exposure control plan, including an exposure determination, 1910.1030(c)
OSHA requires a written plan to eliminate or minimize employee exposure. Covered employers must include:
- An exposure determination per 1910.1030(c)(2);
- A schedule and method of implementing paragraphs (d), (f), (g), and (h) of 1910.1030; and
- A procedure to evaluate circumstances surrounding exposure incidents.
The plan must be reviewed annually and as necessary to reflect changes in tasks, procedures, and positions that affect occupational exposure, as well as technological changes that eliminate or reduce occupational exposure. Annually, employers also must document in the plan that they have:
- Considered and begun using appropriate, commercially-available, effective safer medical devices designed to eliminate or minimize occupational exposure; and
- Solicited input from front-line employees in identifying, evaluating, and selecting effective engineering and work practice controls.
#2 Violation: Failure to provide effective information and training, 1910.1030(g)(2)
Employers must ensure that their employees with occupational exposure receive initial training that covers all elements in paragraph (g)(2) of the standard. This is prior to being placed in positions where occupational exposure may occur. Training must also be offered at least annually thereafter, and when new or modified tasks or procedures affect an employee’s occupational exposure.
However, HIV and HBV laboratory and production facility employees must receive specialized initial training, in addition to the training provided to all employees with occupational exposure.
It’s important (and required) that training be presented at an educational level and in a language that employees understand and that employees have the opportunity to ask the trainer questions. A trainer knowledgeable in the training elements as they relate to the workplace is mandated as well.
#3 Violation: Failure to offer hepatitis B vaccination and post-exposure evaluation and follow-up, 1910.1030(f)
Employers must offer the hepatitis B vaccine to employees with occupational exposure after the employees have received training and within 10 days of initial assignment to a job with occupational exposure. Employees who decline to accept the vaccination must sign the statement in 1910.1030 Appendix A.
If an occupationally exposed employee suffers an exposure incident, then post-exposure evaluation and follow-up must be made available. An “exposure incident” is a specific eye, mouth, other mucous membrane, non-intact skin, or parenteral contact with blood or OPIM. The evaluation and follow-up must be at no cost to the employee and include:
- Documenting the route(s) of exposure and the circumstances under which the exposure incident occurred;
- Identifying and testing the source individual for HBV and HIV infectivity, if the source individual consents or the law doesn’t require consent;
- Collecting and testing the exposed employee’s blood, if the employee consents;
- Offering post-exposure prophylaxis;
- Offering counseling; and
- Evaluating reported illnesses.
After evaluating the employee, the healthcare professional will provide a limited written opinion to the employer, but it will not offer any medical findings or diagnoses.
Key to remember: If you have employees with occupational exposure, you’re covered by the Bloodborne Pathogens standard and must comply with all the requirements outlined in 1910.1030. The top three trouble spots for violators in fiscal years 2023 and 2024 involved the written plan, employee training, and vaccination/evaluation.


See More
RELATED NEWS

NewsIndustry NewsEnforcement and Audits - OSHABloodborne Pathogens Training RequirementsBloodborne Pathogens Prevention and ControlSafety & HealthIn-Depth ArticleGeneral Industry SafetyMaritime SafetyFocus AreaBloodborne PathogensEnglishOSHA Violations and PenaltiesUSA
09/12/2023
Any employer can have a blood spill, but is cleanup covered by 1910.1030?
NewsIndustry NewsEnforcement and Audits - OSHABloodborne Pathogens Training RequirementsBloodborne PathogensSafety & HealthIn-Depth ArticleGeneral Industry SafetyMaritime SafetyFocus AreaBloodborne PathogensEnglishOSHA Violations and PenaltiesUSA
09/12/2023
Any employer can have a blood spill, but is cleanup covered by 1910.1030?

NewsIndustry NewsEnforcement and Audits - OSHABloodborne Pathogens Training RequirementsBloodborne PathogensSafety & HealthIn-Depth ArticleGeneral Industry SafetyMaritime SafetyFocus AreaBloodborne PathogensEnglishOSHA Violations and PenaltiesUSA
01/26/2023
OSHA Bloodborne Pathogens Standard snags violators in industries other than healthcare


Specialized Industries
Go beyond the regulations! Visit the Institute for in-depth guidance on a wide range of compliance subjects in safety and health, transportation, environment, and human resources.
J. J. Keller® COMPLIANCE NETWORK is a premier online safety and compliance community, offering members exclusive access to timely regulatory content in workplace safety (OSHA), transportation (DOT), environment (EPA), and human resources (DOL).

Interact With Our Compliance Experts
Puzzled by a regulatory question or issue? Let our renowned experts provide the answers and get your business on track to full compliance!

Upcoming Events
Reference the Compliance Network Safety Calendar to keep track of upcoming safety and compliance events. Browse by industry or search by keyword to see relevant dates and observances, including national safety months, compliance deadlines, and more.
SAFETY & COMPLIANCE NEWS
Keep up with the latest regulatory developments from OSHA, DOT, EPA, DOL, and more.



REGSENSE® REGULATORY REFERENCE
Explore a comprehensive database of word-for-word regulations on a wide range of compliance topics, with simplified explanations and best practices advice from our experts.

THE J. J. KELLER INSTITUTE
The Institute is your destination for in-depth content on 120+ compliance subjects. Discover articles, videos, and interactive exercises that will strengthen your understanding of regulatory concepts relevant to your business.



ADD HAZMAT, ENVIRONMENTAL, & HR RESOURCES
Unlock exclusive content offering expert insights into hazmat, environmental, and human resources compliance with a COMPLIANCE NETWORK EDGE membership.

DIRECT ACCESS TO COMPLIANCE EXPERTS
Struggling with a compliance challenge? Get the solution from our in-house team of experts! You can submit a question to our experts by email, set up a phone or video call, or request a detailed research report.



EVENTS
Register to attend live online events hosted by our experts. These webcasts and virtual conferences feature engaging discussions on important compliance topics in a casual, knowledge-sharing environment.
Most Recent Highlights In Environmental

NewsIndustry NewsIndustry NewsPesticidesPesticide Registration and LabelingEnvironmental Protection Agency (EPA)EnvironmentalEnglishFocus AreaPesticidesUSA
2026-07-01T05:00:00Z
EPA sets MyPeST compliance reporting deadlines for bilingual pesticide labeling requirements
The Environmental Protection Agency (EPA) published instructions and deadlines for pesticide registrants to report compliance with bilingual labeling requirements in the MyPeST application. The first compliance reporting deadline is July 31, 2026, for pesticide products with the highest toxicity.
Who’s impacted?
Compliance reporting applies to registrants of pesticide products subject to the bilingual labeling requirements established by the Pesticide Registration Improvement Act of 2022 (PRIA 5) amendments to the Federal Insecticide, Fungicide, and Rodenticide Act (FIFRA).
PRIA 5 requires all end-use pesticide product labels to provide Spanish translations of the human health and safety sections by including the translated sections directly on the label or providing a link via scannable technology or other readily accessible electronic methods to the translated sections. EPA allows certain antimicrobial and non-agricultural pesticide products to comply by providing access to Spanish-language Safety Data Sheets instead of direct label translations.
Compliance timelines are based on the type of pesticide and its toxicity category.
What’s required?
Pesticide registrants must report compliance with the PRIA 5 bilingual labeling requirements using EPA’s MyPeST app. The agency recently published detailed reporting instructions in the MyPeST Application User Guide (accessible in the MyPeST app).
EPA also established the following deadlines for reporting compliance in MyPeST:
| Pesticide product type | Bilingual labeling deadline | Compliance reporting deadline |
|---|---|---|
| Restricted use pesticides (RUPs) | December 29, 2025 | July 31, 2026 |
| Non-RUP agricultural products | ||
| Acute Toxicity Category I | December 29, 2025 | July 31, 2026 |
| Acute Toxicity Category II | December 29, 2027 | January 28, 2028 |
| Antimicrobials and non-agricultural products | ||
| Acute Toxicity Category I | December 29, 2026 | January 28, 2027 |
| Acute Toxicity Category II | December 29, 2028 | January 28, 2029 |
| All other pesticide products | December 29, 2030 | January 28, 2031 |

NewsIndustry NewsEnvironmental Protection Agency (EPA)Oil Spill PreventionOil Spill PreventionEnvironmentalIn-Depth ArticleCWA ComplianceEnglishFocus AreaUSA
2026-06-30T05:00:00Z
Secondary containment alternative: Does your oil-filled operational equipment qualify?
Facilities that run like a well-oiled machine often rely on just that — operational equipment that stores and uses oil to function (like hydraulic systems). But wherever oil is stored, there’s always the possibility of a leak, and spilled oil can do serious harm, especially if it reaches water.
That’s where the Environmental Protection Agency’s (EPA’s) Spill Prevention, Control, and Countermeasure (SPCC) rule comes in. Usually, regulated facilities must equip oil-filled operational equipment with general secondary containment, which is designed to temporarily hold discharged oil until it can be properly cleaned up. However, some facilities may have another compliance option available.
EPA offers an alternative to secondary containment for qualified oil-filled operational equipment. Let’s take a look at the eligibility criteria and what the other method of compliance requires.
What’s oil-filled operational equipment?
EPA defines “oil-filled operational equipment” at 40 CFR 112.2. Generally, it refers to equipment that has one or more oil storage containers with oil that’s used solely to operate the equipment. Common examples are lubrication systems for pumps and compressors, machining coolant systems, circuit breakers, and electrical switches.
Does your facility have qualified equipment?
Only qualified oil-filled operational equipment is eligible for the alternative requirements to general secondary containment.
The SPCC rule considers oil-filled operational equipment to be qualified if it hasn’t had one discharge of oil exceeding 1,000 gallons or two discharges of oil exceeding 42 gallons each over the following time periods:
- If the facility has operated for at least 3 years, within any 12-month period in the 3 years before the SPCC Plan’s certification date; or
- If the facility has operated for less than 3 years, since becoming subject to the SPCC regulations.
Take note! When determining whether your facility’s oil-filled operational equipment is eligible under federal standards:
- Don’t count oil discharges caused by natural disasters, acts of war, or terrorism; and
- Don’t count the total amount of oil spilled, only the amount that reaches navigable waters or adjoining shorelines.
What about oil-filled manufacturing equipment?
The SPCC rule distinguishes between oil-filled manufacturing equipment and oil-filled operational equipment. Oil-filled manufacturing equipment stores oil only as a supporting element for conducting a mechanical or chemical operation to create or modify a product. It typically involves a flow-through process in which oil continuously moves through the equipment. Examples of this type of equipment include reaction vessels, mixing tanks, and distillation columns.
Because it’s defined independently under the SPCC rule, oil-filled manufacturing equipment isn’t eligible for the alternative compliance option available to qualified oil-filled operational equipment.
What are the alternative measures?
Instead of providing secondary containment for qualified oil-filled operational equipment, facilities may choose to comply with the alternative requirements at 112.7(k), which include:
- Establishing and documenting an inspection or a monitoring program to detect equipment failures and discharges; and
- Adding to the SPCC Plan:
- An oil spill contingency plan according to the requirements of Part 109; and
- A written commitment of the resources (manpower, equipment, and materials) needed to quickly control and remove any potentially harmful quantities of discharged oil;
Take note! If your business must submit a facility response plan (FRP) under 112.20, the oil spill contingency plan and written commitment requirements don’t apply since your FRP already contains these elements.
Why should my facility consider the alternative compliance option?
The alternative requirements to general secondary containment don’t require facilities to prepare an impracticability determination for qualified oil-filled operational equipment.
The impracticability determination provisions at 112.7(d) impose more requirements for facilities that use alternative measures to secondary containment for unqualified equipment.
In addition to meeting the same requirements for qualified oil-filled operational equipment, facilities must have the oil spill contingency plan certified by a Professional Engineer (unless self-certifying as a qualified facility). They also must:
- Describe in the SPCC Plan the reasons such measures aren’t practicable, and
- Conduct periodic integrity tests of bulk storage containers and periodic integrity and leak tests of valves and piping.
Key to remember: The SPCC rule offers an alternative to general secondary containment requirements for qualified oil-filled operational equipment.

NewsGreenhouse GasesAir QualityExcavationsToxic Substances Control Act - EPAToxic Subtances Control Act - EPAPersonal Protective EquipmentAir EmissionsTSCA ComplianceExcavationsMonthly Roundup VideoMiningCAA ComplianceUSAEnglishIndustry NewsSafety & HealthConstruction SafetyInfectious DiseasesCOVID-19General Industry SafetyGeneral Duty ClauseSpecialized IndustriesEnvironmentalFocus AreaRespiratory ProtectionMine SafetyGeneral Duty ClauseAir ProgramsVideo
EHS Monthly Round Up - August 2025
In this August 2025 roundup video, we'll review the most impactful environmental health and safety news.
Hi everyone! Welcome to the monthly news roundup video, where we’ll review the most impactful environmental health and safety news. Let’s take a look at what’s happened over the past month!
OSHA extended the comment period for multiple proposed rules it published on July 1. Stakeholders now have an extra 60 days, until November 1, to comment. Impacted rules include those for respiratory protection, construction illumination, COVID-19, and the General Duty Clause.
OSHA is expanding its Voluntary Protection Programs to help employers develop strong safety programs and lower injury rates. To participate, employers must submit an application to OSHA and undergo an onsite evaluation by a team of safety and health professionals.
Following a series of recent trench collapses, OSHA urges employers to take steps to protect workers. Trench collapses can be prevented by sloping or benching trench walls at an angle, shoring trench walls with supports, and shielding walls with trench boxes. More information can be found on OSHA’s website.
The Mine Safety and Health Administration launched a webpage for its new Compliance Assistance in Safety and Health, or CASH, program. The agency anticipates a surge in domestic mining productivity and seeks to proactively provide miners and mine operators with compliance assistance materials.
Turning to environmental news, EPA proposes challenges to California’s Clean Truck Check program. The program aims to reduce emissions of nitrogen oxides and particulate matter for heavy-duty vehicles. EPA supports the regulation as it applies to California-registered vehicles but disapproves the regulation as it applies to out of state and out of country vehicles. Stakeholders have until September 25 to comment on the proposal.
On August 14, EPA released the July 2025 nonconfidential TSCA Inventory of chemical substances manufactured, processed, or imported in the U.S. The Inventory contains over 86 thousand chemicals, nearly half of which are in active use. The next inventory update is planned for late 2026.
And finally, EPA proposes to rescind the 2009 Endangerment Finding and repeal greenhouse gas emissions for new motor vehicles and vehicle engines. The agency will accept comments on the proposal through September 15.
Thanks for tuning in to the monthly news roundup. We’ll see you next month!

NewsHazardous WasteGreenhouse GasesWaste ManifestsWater ProgramsFall ProtectionMonthly Roundup VideoFall Protection for ConstructionCAA ComplianceUSAWater ProgramsWaste/HazWasteEnglishIndustry NewsSafety & HealthConstruction SafetyGeneral Industry SafetyWasteEnvironmentalFocus AreaAir ProgramsVideo
EHS Monthly Round Up - September 2025
In this September 2025 roundup video, we'll review the most impactful environmental health and safety news.
Hi everyone! Welcome to the monthly news roundup video, where we’ll review the most impactful environmental health and safety news. Let’s take a look at what’s happened over the past month.
OSHA released its Spring 2025 regulatory agenda on September 4. Many rulemakings have been pushed into the fourth quarter of 2025 and the first half of 2026, while a few have been removed from the agenda altogether. These include Infectious Diseases, Blood Lead Level for Medical Removal, and the Musculoskeletal Disorders Column on the OSHA 300 log.
Three rules moved into the long-term actions category – Workplace Violence in Health Care and Social Assistance, Cranes and Derricks in Construction, and Process Safety Management and Prevention of Major Chemical Accidents. The proposed rule stage saw an influx of new entries, most of which were published in the July 1 Federal Register.
The Standards Improvement Project, slated for proposal in May 2026, intends to “remove, modernize, or narrow duplicative, unnecessary, or overly burdensome regulatory provisions.”
OSHA renewed its alliance with the National Waste and Recycling Association and the Solid Waste Association of North America. The partnership will focus on safety issues such as transportation hazards; slips, trips, and falls; needlestick and musculoskeletal injuries; and health issues associated with lithium battery hazards in waste/recycling collection and processing.
For the 15th year in a row, fall protection for construction topped OSHA’s list of top 10 violations. In fiscal year 2024, there were 5,914 recorded fall protection violations, down from 7,271 in fiscal year 2023. The standards that round out the top 10 remain unchanged, with a shift in some of the rankings.
Turning to environmental news, EPA proposes to eliminate the Greenhouse Gas Reporting Program requirements for all source categories except the petroleum and natural gas systems category. The agency also proposes to suspend compliance obligations for covered facilities until 2034. A public hearing was held October 1 and stakeholders have until November 3 to comment on the proposal.
Hazardous waste handlers may continue to use 5-paper copy manifest forms. EPA announced it will accept these forms from entities regulated by the Resource Conservation and Recovery Act, or RCRA, until further notice. The agency will give a 90-day notice before it plans to stop accepting the 5-copy forms.
And finally, EPA published its Spring 2025 regulatory agenda on September 4. The agenda outlines the agency’s upcoming regulatory actions and their status in the rulemaking process. Major updates on the docket include those for greenhouse gases, risk management rules, and the Renewable Fuel Standards for 2026 and 2027.
Thanks for tuning in to the monthly news roundup. We’ll see you next month!

NewsHazardous WasteEnforcement and Audits - OSHAToxic Substances Control Act - EPAToxic Subtances Control Act - EPAElectronic Reporting of Injury and Illness RecordsTSCA ComplianceMonthly Roundup VideoCAA ComplianceUSAInjury and Illness RecordkeepingWaste/HazWasteEnglishOSHA Violations and PenaltiesIndustry NewsCrystalline SilicaWaste HandlersSafety & HealthGeneral Industry SafetyWasteWaste TransportersEnvironmentalFocus AreaToxic and Hazardous Substances - OSHAVideo
EHS Monthly Round Up - January 2025
In this January 2025 monthly roundup video, we'll review the most impactful environmental health and safety news.
Hi everyone! Welcome to the monthly news roundup video, where we’ll review the most impactful environmental health and safety news. There’s a lot going on, so let’s get started!
As happens at the start of most incoming presidential administrations, a freeze has been placed on all regulatory activity at the federal level, giving the new administration time to review agencies’ plans. The Office of Management and Budget, which must approve most rulemaking activities, has sent numerous pending rules back to the agencies for review. In addition, OSHA withdrew its infectious diseases proposed rule and its COVID-19 in healthcare rule prior to the inauguration.
OSHA’s penalties increased on January 15. The maximum penalty amounts for serious and other-than-serious violations increased to $16,550. For willful or repeated violations, the maximum penalty increased to $165,514 per violation.
OSHA updated its directive on injury and illness recordkeeping policies and procedures. While it’s intended for OSHA compliance officers, employers can use the information to help with recordkeeping compliance.
Fewer workers died on the job in 2023, as fatal work injuries decreased 3.7 percent from 2022. Transportation incidents remained the most frequent type of fatal event, accounting for over 36 percent of all occupational fatalities.
California’s Occupational Safety and Health Standards Board voted to adopt a permanent silica standard. If approved, it would extend and strengthen the state’s emergency temporary standard, which was put in place in December 2023.
The National Institute for Occupational Safety and Health updated its List of Hazardous Drugs in Healthcare Settings. This is a resource for employers and employees in identifying drugs that are hazardous to the health and safety of those who handle them.
Turning to environmental news, EPA released the biannual update of the nonconfidential TSCA inventory. The inventory helps facilities determine their regulatory requirements for the chemicals they use or plan to use.
And finally, EPA added new Management Method Codes to describe how hazardous waste will be managed after temporary storage and transfer. As of January 1st, hazardous waste handlers must use the codes on the Biennial Report Waste Generation and Management forms.
Thanks for tuning in to the monthly news roundup. We’ll see you next month!
Most Recent Highlights In Transportation

NewsProcess Safety ManagementEnforcement and Audits - OSHAToxic Substances Control Act - EPAWasteErgonomicsMonthly Roundup VideoUSAWaste/HazWasteEnglishErgonomicsIndustry NewsEnforcement and Audits - OSHASafety & HealthToxic Substances - EPAGeneral Industry SafetyWasteEnvironmentalHazardous Materials Safety - OSHAFocus AreaVideo
EHS Monthly Round-Up - August 2024
In this August 2024 roundup, we'll review the most impactful environmental, health, and safety news.
Hi everyone! Welcome to the monthly news roundup video, where we’ll review the most impactful environmental, health, and safety news. Please view the content links in the transcript for more information about the topics I’ll be covering today. Let’s get started!
Two State Plan agencies allegedly provided advance notice of workplace inspections to employers, a practice that’s prohibited under the Occupational Safety and Health Act. Now, lawmakers have requested that the Department of Labor’s acting secretary address the allegations and explain what challenges OSHA faces when monitoring and enforcing State Plan compliance.
A recent study shows jobs in agriculture, forestry, fishing, and hunting are among California’s most dangerous, accounting for the highest number of fatalities among full-time workers. Transportation and utilities jobs ranked second and construction was third.
Remote isolation of process equipment can quickly stop the release of hazardous materials, which can help prevent fatalities and injuries, limit facility damage, and better protect communities and the environment. A U.S. Chemical Safety Board study explores their use and makes recommendations for their utilization in chemical facilities.
A National Safety Council report explores the role of diversity, equity, and inclusion on work-related musculoskeletal disorders, or MSDs. MSDs are the most common workplace injury and often lead to worker disability, early retirement, and employment limitations.
And finally, turning to environmental news, EPA published a final rule that revises its hazardous waste export manifest regulations. All hazardous waste shipments and manifest-related reports will be managed electronically through the agency’s e-Manifest program.
Thanks for tuning in to the monthly news roundup. We’ll see you next month!
NewsIndustry NewsEnglishIn-Depth ArticleCAA ComplianceSustainabilityEnvironmental Management SystemsCWA ComplianceEnvironmentalWaste/HazWasteSustainabilityESG (Environmental, Social, and Governance)Focus AreaUSA
2026-06-26T05:00:00Z
Multimedia inspections are back: How to prepare for comprehensive EPA and state audits
Regulators have returned to routine, in-person inspections, and many are no longer limited to a single program. The Environmental Protection Agency (EPA) and state agencies are again conducting multimedia inspections that review air, water, and hazardous waste compliance in one visit. For facilities, this shift raises the stakes. An issue in one program can quickly lead inspectors into others, especially when records or operations don't align.
Most inspectors now arrive with background data already reviewed. Electronic submissions, air reports, discharge monitoring reports, and hazardous waste filings are compared against what they see on-site. When numbers, dates, or practices don't match, the scope of the inspection often expands.
What inspectors are really evaluating
While documents are important, inspectors focus on whether procedures match actual operations. They will often start with a walk-through of the facility, tracing how materials move through production and become emissions, discharges, or wastes.
For example:
- Air compliance may be checked by reviewing fuel use, hours of operation, or control device logs;
- Stormwater compliance often involves visual checks for exposed materials and conditions of controls; and
- Hazardous waste inspections typically focus on labeling, container condition, and accumulation practices.
The common thread is consistency. If a plan says one thing but operators do another, it's likely to result in a finding.
Common gaps seen during multimedia inspections
Across industries, several issues appear repeatedly:
- Records that don't match across programs (e.g., waste logs versus manifests);
- Missing or incomplete inspection logs for air or stormwater systems;
- Assumptions about exemptions without supporting documentation;
- Satellite accumulation areas managed informally outside environmental oversight; and
- Housekeeping issues that create unintended stormwater exposure.
Many of these aren't complex violations. They're breakdowns in communication, training, or follow-through.
A practical way to prepare
Facilities can improve readiness by conducting an internal, cross-media review that mirrors an actual inspection. This is more effective than reviewing each program in isolation.
Start with a process-based walk-through:
- Identify where raw materials enter the facility.
- Follow how they're used, stored, and handled.
- Note where wastes, emissions, or discharges are generated.
- Confirm how each is managed and documented.
At each step, ask two questions:
- Is this activity reflected accurately in our records and plans?
- Would an operator explain it the same way it's written?
This approach often reveals gaps that aren't obvious during a desk review.
A recent case: How one issue expands the scope
At a mid-sized manufacturing facility, inspectors began with a routine hazardous waste review. They noticed that waste logs showed periodic disposal of solvent residues, but there were no related air records for emissions tied to cleaning operations.
This led inspectors to review the facility’s air permit assumptions. They found that solvent use had increased over time, but the facility hadn't updated its potential-to-emit calculations. What started as a simple waste review expanded into an air applicability concern.
The facility ultimately faced findings in both programs, not because of a single major violation, but because information didn't align across systems.
Strengthening compliance across programs
Preparation doesn't require building new systems. It requires making sure existing ones are aligned and consistently followed.
Focus on:
- Clear ownership of compliance tasks across departments;
- Regular cross-checks between records (air, water, waste);
- Training staff on how their daily tasks affect compliance; and
- Maintaining documentation that supports assumptions, exemptions, and limits.
Facilities that treat compliance as a connected system, not separate programs, are better positioned during inspections.
Key to remember: A multimedia inspection looks for consistency across air, water, and waste programs, not just isolated compliance. If your records and operations tell the same story, you're far less likely to face expanded scrutiny.
NewsHazardous WasteIndustry NewsWaste GeneratorsEnglishWasteEnvironmentalIn-Depth ArticleWaste/HazWasteFocus AreaUSA
2026-06-25T05:00:00Z
Hazardous waste episodic events: What to do when a bad month happens
Every generator has that month. A tank clean-out gets scheduled; a forklift punctures a tote, and suddenly you've generated way more hazardous waste than you normally would. If you're a Very Small Quantity Generator (VSQG) or Small Quantity Generator (SQG), that one bad month could technically bump you into Large Quantity Generator (LQG) status, potentially subjecting the facility to LQG requirements such as contingency planning, personnel training, and biennial reporting.
The good news is that EPA built in an escape hatch. The 2016 Generator Improvements Rule added 40 CFR Part 262, Subpart L (the "episodic event" provision), which lets you keep your normal generator category for that month, if you follow the rules in 40 CFR 262.232 exactly.
Scenario 1: The planned tank clean-out
Picture a metal finishing shop that's normally an SQG, generating about 400 kg/month of spent plating solution. They finally get around to cleaning out an old process tank that's been sitting idle for three years. That clean-out produces about 1,800 kg of sludge in one shot and enough to push them into LQG numbers for the month.
Since this is something the facility planned and scheduled for, it's a planned episodic event. Here's what the employer would need to do:
- Notify EPA (or the delegated state agency) at least 30 calendar days before the clean-out starts, using EPA Form 8700-12. Include the start/end dates, why the event is happening, estimated waste types and quantities, and a 24-hour emergency contact.
- Double-check the facility's EPA ID number to make sure it is current.
- Stage the waste properly with compliant containers or tanks and labeled with the episodic event start date.
- Get it manifested and shipped off-site within 60 calendar days of the start date.
- Hang onto every record including the notification, manifests for 3 years after the event ends.
Scenario 2: The unplanned spill
Next, picture a packaging plant. They are a VSQG generating around 80 kg/month. They have a forklift punch a hole in a 275-gallon tote of listed solvent and by the time cleanup is done, they're looking at about 900 kg of contaminated absorbent and solvent residue. Nobody planned this. It's not part of normal operations. That makes it an unplanned episodic event. Here is what they should do:
- They have 72 hours to notify EPA or the state by phone, email, or fax. There will be no time to fill out paperwork first.
- Follow that up by submitting EPA Form 8700-12 after the fact, documenting what happened since you couldn't give advance notice.
- Keep the spill cleanup waste separate from your routine waste streams and label it with the episodic start date.
- The same 60-day shipping window and 3-year recordkeeping requirement apply here too.
The things you can't skip
Whether the event is planned or unplanned, there are a handful of conditions that apply across the board and missing any one of them could cost you the episodic event relief entirely.
- One event per year, period. Both VSQGs and SQGs get exactly one episodic event a year unless they petition the Regional Administrator under 40 CFR 262.233 for a second. That second one must be the opposite type, so if your first was planned, the next must be unplanned.
- The clock doesn't wait. Exactly 30 days out for planned and 72 hours for unplanned are required. Miss either window or you lose the relief entirely, meaning full LQG status kicks in for that period.
- The 60-day shipping clock starts on day one of the event, not when you send the notification, so make sure to track it immediately.
- Manifest the waste properly. Episodic waste can ship under the standard Subpart B manifest rules, even in the same load as your regular waste.
- Write everything down. Three years of solid records such as dates, causes of event, quantities, and where it went is what separates a clean inspection from an enforcement headache.
Keys to remember: The episodic event provision rewards generators who plan, classify the event correctly, notify on time, ship within 60 days, and document everything for three years.
NewsGreenhouse GasesAir QualityAir EmissionsChange NoticesChange NoticeVirginiaCAA ComplianceEnvironmentalFocus AreaEnglishAir ProgramsAir Programs
2026-06-24T05:00:00Z
Virginia reinstates power plant CO2 budget program
Effective date: April 24, 2026
This applies to: Power plant owners
Description of change: The Virginia Department of Environmental Quality reinstated the Virginia CO2 Budget Trading Program Regulation, which implements the Regional Greenhouse Gas Initiative (RGGI). Participation in the RGGI was stopped in 2023, but the state will resume participation on July 1, 2026, the same date on which the compliance requirements take effect.
The regulation requires fossil fuel-fired units that serve an electricity generator with a capacity of 25 megawatts or more to obtain enough allowances to cover CO2 emissions, which they can purchase in the September and December RGGI auctions.
The department also adopted amendments to the regulations, including establishing a one-time 6-month control period from July 1, 2026, to December 31, 2026.
Related state info: Clean air operating permits state comparison
NewsMunicipal WastewaterChange NoticesChange NoticeWater ProgramsEnvironmentalCWA ComplianceEnglishFocus AreaNorth Carolina
2026-06-24T05:00:00Z
North Carolina approved revisions to wastewater discharge rules
Effective date: May 1, 2026
This applies to: Facilities with domestic wastewater discharges up to 2 million gallons per day
Description of change: The North Carolina Department of Environmental Quality (DEQ) adopted a rule that adds a permitting option to the National Pollutant Discharge Elimination System (NPDES) program for facilities with domestic wastewater discharges of up to 2 million gallons per day.
DEQ removed the ban on new or expanded discharges of oxygen-consuming waste when the 7Q10 and 30Q2 flows are both 0 for these facilities. In other words, it allows systems to discharge domestic wastewater to zero-flow receiving streams, provided the system:
- Meets qualifying criteria,
- Complies with specific effluent limits, and
- Uses low-energy methods before discharging wastewater to the receiving stream.
It’ll likely benefit areas where the cost of piping to a higher-flowing stream farther away is prohibitive.
Most Recent Highlights In Safety & Health
NewsGroundwaterSafe Drinking WaterWater ProgramsWater QualityWater ProgramsCWA ComplianceEnglishMunicipal WastewaterWater PermittingChange NoticesChange NoticeWater ReportingIndustrial WastewaterEnvironmentalNew HampshireFocus Area
2026-06-24T05:00:00Z
New Hampshire updates sludge management rules
Effective date: May 15, 2026
This applies to: Owners and operators of drinking water and wastewater treatment plants that generate sludge; land application sites; and facilities that treat, manage, or dispose of sludge
Description of change: The New Hampshire Department of Environmental Services amended sludge management rules. Major changes include:
- Reinstating 5-year site and facility permit renewals (instead of 10 years),
- Adding annual reporting requirements for sludge haulers (which already apply to septage haulers), and
- Requiring all applications to be submitted electronically.
The rule also codifies per- and polyfluoroalkyl substances (PFAS) sampling (implemented in 2019 for the sludge quality certificate program).
NewsGroundwaterToxic/Hazardous Substance ReleasesCERCLA, SARA, EPCRASafe Drinking WaterChange NoticesChange NoticeWater ProgramsNew JerseyEnvironmentalCWA ComplianceEnglishFocus Area
2026-06-24T05:00:00Z
New Jersey adopts permanent remediation standards for PFAS
Effective date: June 15, 2026
This applies to: Contaminated sites subject to the remediation regulations for contaminated groundwater, soil, and soil leachate
Description of change: The New Jersey Department of Environmental Protection (NJDEP) formally adopted its interim remediation standards for specific per- and polyfluoroalkyl substances (PFAS), including:
- Groundwater quality standards for hexafluoropropylene oxide dimer acid and its ammonium salt (GenX chemicals); and
- Soil and soil leachate remediation standards for:
- Perfluorononanoic acid (PFNA);
- Perfluorooctane sulfonate (PFOS);
- Perfluorooctanoic acid (PFOA);
- GenX chemicals; and
- Methanol.
The interim standards have been in place since 2022 and 2023, requiring regulated entities to conduct remediation to ensure these PFAS are cleaned up.
Additionally, the NJDEP amended the technical requirements to mandate analyses of the following chemicals in all media when contaminants are unknown or not well documented at a contaminated site:
- PFNA,
- PFOS,
- PFOA,
- GenX chemicals, and
- 2,3,7,8-tetrachlorodibenzo-p-dioxin.
NewsHazardous WasteWaste HandlersChange NoticesChange NoticeWasteWaste/HazWasteWaste ManagementEnvironmentalNevadaEnglishFocus Area
2026-06-24T05:00:00Z
Nevada adds requirements for hazardous waste recyclers
Effective date: June 8, 2026
This applies to: Hazardous waste recyclers
Description of change: The State Environmental Commission adopted regulations to add requirements for entities that recycle certain hazardous waste, including compliance with:
- Certain federal requirements;
- Local zoning requirements, if applicable;
- Specific reporting and notification requirements; and
- Other particular regulations of the commission.
The rules also:
- Exempt owners and operators of certain facilities that recycle certain hazardous materials without storing those materials before they’re recycled from the above requirements, and
- Add fees for written determinations (required to construct or operate a facility or mobile unit for hazardous waste recycling) and for the facilities that recycle certain hazardous materials without storing those materials before they’re recycled.
NewsToxic Substances Control Act - EPAChange NoticesChange NoticeTSCA ComplianceToxic Substances - EPACaliforniaEnvironmentalEnglishFocus Area
2026-06-24T05:00:00Z
California adds TPhP nail products to Priority Products list
Effective date: October 1, 2026
This applies to: Nail products containing triphenyl phosphate (TPhP) at concentrations greater than 250 parts per million (ppm)
Description of change: The California Department of Toxic Substances Control added nail products with concentrations of 250 ppm or more of TPhP to the Priority Product list, making the substance subject to the Safer Consumer Products (SCP) Regulations.
By November 30, 2026, manufacturers must submit a Priority Product Notification. By March 30, 2027, manufacturers must submit:
- A Chemical Removal Intent/Confirmation Notification,
- A Product Removal Intent/Confirmation Notification,
- A Product-Chemical Replacement Intent/Confirmation Notification, or
- A Preliminary Alternatives Analysis Report or alternate reporting options.
NewsIndianaSafe Drinking WaterChange NoticesChange NoticeWater ProgramsEnvironmentalCWA ComplianceEnglishUnderground Injection ControlFocus Area
2026-06-24T05:00:00Z
Indiana adds permanent underground carbon dioxide storage rules
Effective date: June 10, 2026
This applies to: Entities that seek to participate in carbon sequestration projects
Description of change: The Natural Resources Commission adopted rules for permanent underground carbon dioxide storage, establishing:
- The rules for entities seeking to petition the Indiana Department of Natural Resources to issue involuntary integration orders for pore spaces, and
- The rules for storage operators seeking to apply for certificates of project completion.
These regulations add options for entities; the requirements apply only if the options are utilized.
The rules impact entities seeking to participate in carbon sequestration projects. The regulations also affect pore space owners and surface owners.
Most Recent Highlights In Human Resources
NewsTier II Inventory ReportingIndustry NewsIndustry NewsCERCLA, SARA, EPCRAEnvironmental Protection Agency (EPA)Safety Data Sheet ReportingEnvironmentalEnglishSARA ComplianceFocus AreaUSA
2026-06-24T05:00:00Z
EPA aligns EPCRA rules with OSHA’s HazCom amendments
The Environmental Protection Agency (EPA) published a final rule on June 22, 2026, conforming the hazardous chemical inventory reporting regulations under the Emergency Planning and Community Right-to-Know Act (EPCRA) to the Occupational Safety and Health Administration’s (OSHA’s) Hazardous Communication (HazCom) standard amendments of 2012 and 2024.
Who’s covered?
The final rule applies to facilities regulated under EPCRA Sections 311 and 312. These facilities are:
- Required by OSHA’s HazCom standard to maintain Safety Data Sheets (SDSs) for hazardous chemicals on-site at or above the reporting threshold, and
- Required by EPA’s EPCRA Section 312 rules (40 CFR Part 370) to submit annual hazardous chemical inventory reports (commonly known as Tier II reports) for the same chemicals by March 1.
Covered facilities submit SDSs and annual inventory reports to the State Emergency Response Commission (SERC), Local Emergency Planning Committee (LEPC), and local fire department.
How does this impact facilities?
EPA’s final rule replaces the previous EPCRA hazard categories with OSHA’s GHS-aligned hazard classes and hazard categories (totaling 118), which are already used in SDSs. Facilities must use OSHA’s hazard classes with their categories for SDS submissions and hazardous chemical inventory reports required under EPCRA Sections 311 and 312.
Note: SDSs for substances already contain the updated hazard classes and hazard categories. SDSs for mixtures must incorporate them by November 2027.
What’s the compliance timeline?
Covered facilities must use the new hazard categories by January 1, 2028. EPA expects facilities to incorporate them into the reporting year 2027 Tier II report (due March 1, 2028).
Key to remember: EPA has aligned regulations under EPCRA Sections 311 and 312 with OSHA’s HazCom amendments for hazardous chemical reporting requirements.
NewsProcess Safety ManagementRisk Management ProgramRisk Management ProgramCAA ComplianceIn-Depth ArticleEnglishSafety Data SheetsIndustry NewsSafety & HealthGeneral Industry SafetyGeneral Duty ClauseEnvironmentalFocus AreaHazardous Materials Safety - OSHAHazard CommunicationGeneral Duty ClauseAir ProgramsUSA
2026-06-23T05:00:00Z
CSB mounts pressure on OSHA, EPA over deadly process safety gap
Sugar may seem pretty harmless. However, a deadly explosion at a Kentucky caramel coloring facility reveals how this assumption can lead to disaster. The Chemical Safety and Hazard Investigation Board (CSB) is again urging OSHA and EPA to address a gap in their chemical safety regulations.
The board is calling for them to tackle “reactive hazards.” These are the hazards CSB says triggered the tragedy. The familiar message has been repeated since 2002, but the alarm bells grow louder and more urgent now. These warnings are not just for OSHA and EPA. They are also for chemical plants and food ingredient manufacturers. Despite not being covered in the process safety and risk management standards, reactive hazards can and have led to catastrophe.
Runaway reaction
CSB determined that the explosion happened when a 2,500-gallon reactor experienced a runaway decomposition reaction. The reaction involved an “invert sugar” ingredient used to make caramel coloring. It rapidly increased the temperature and pressure. Then it overwhelmed the reactor’s emergency pressure relief system.
The reactor ruptured violently. Two workers died when the blast damaged a control room 40 feet from the reactor. Debris from the incident traveled as far as 400 feet beyond the facility fence line. It also caused approximately $40 million in damage.
CSB found that the reactor’s emergency pressure relief system would have needed to be about four times larger. This would have allowed it to safely relieve pressure generated during the runaway reaction.
Failure to recognize the hazard
CSB’s investigation found that the company did not understand the severe reactive hazards associated with the sugar ingredient. According to the board, this failure contributed to an undersized pressure relief system. It also created confusion on the day of the incident about the increasing pressure.
The report further states that the company’s lack of knowledge stemmed from:
- An incomplete investigation of the ingredients’ reaction potential,
- A lack of industry guidance on the safe manufacture of caramel coloring, and
- No warning on the safety data sheet (SDS) of reaction hazards.
SDS lacked critical information
The board found that the SDS provided by the sugar manufacturer did not warn of its reactivity hazards. CSB concluded that safety information communicated in sugar ingredient SDSs can vary significantly among suppliers. The board noted that improved hazard information in SDSs can help prevent future sugar decomposition incidents. CSB is urging industry groups and suppliers who manufacture invert sugar or corn syrup to update their SDSs for decomposition hazards.
Known regulatory gap
The report emphasizes a gap in:
- OSHA 29 CFR 1910.119, Process Safety Management of Highly Hazardous Chemicals (PSM); and
- EPA 40 CFR 68, Chemical Accident Prevention Provisions, also known as the Risk Management Program (RMP).
That gap is a lack of coverage of facilities processing chemicals with reactive hazards that could have catastrophic consequences.
The Kentucky caramel coloring plant was not subject to PSM and RMP. Had the facility been required to implement either regulation, the reactor designers would have had a better opportunity to be aware of the sugar ingredients’ decomposition hazards, says CSB. The board argues that this may have resulted in a safer design of the emergency pressure relief system.
Repeated recommendations
Since 2002, CSB has reiterated its recommendations for OSHA and EPA to fill the regulatory gap. Neither agency has implemented those recommendations.
Over that same period, the board investigated 15 additional incidents involving reactive chemicals not covered by PSM and RMP. Those incidents resulted in 31 fatalities and hundreds of injuries.
CSB is not deterred
CSB again recommends that OSHA and EPA broaden the coverage of PSM and RMP, respectively, to achieve more comprehensive control of reactive hazards.
Both OSHA and EPA currently use chemical lists to identify the processes subject to coverage. However, CSB claims the two agencies did not adequately consider reactive chemical hazards when developing those chemical lists. As a result, many reactive chemicals are currently not covered.
Word for employers and safety professionals
The latest report highlights the need for:
- Facilities to review not just the SDS for their chemicals but also additional sources of information about their reactive hazards.
- Chemical plants and food manufacturers to address reactive hazards regardless of coverage under 1910.119 and Part 68. At a minimum, these facilities may already be required to meet OSHA’s General Duty Clause and EPA’s Clean Air Act General Duty Clause.
Key to remember
The latest CSB report taps OSHA and EPA to address reactivity hazards. It is also a wake-up call for facilities to understand their reactive chemical hazards. What’s more, the report calls on chemical and food ingredient manufacturers to revisit their SDSs regarding reactive hazards.
NewsIndustry NewsWaste IdentificationEnglishWasteWaste ManagementEnvironmentalIn-Depth ArticleWaste/HazWasteFocus AreaUSA
2026-06-18T05:00:00Z
Hazardous waste determinations in practice: Lessons from aerosols, residues, and empty containers
Hazardous waste determinations remain one of the most common sources of noncompliance under RCRA. The requirement is simple on paper. Generators must determine whether a material is a hazardous waste at the point of generation. In practice, facilities often struggle with how the rules apply to everyday situations. Aerosol cans, process residues, and empty containers are frequent gray areas that lead to inconsistent decisions, inspection findings, and, in some cases, enforcement.
At the core, the regulatory expectation is clear: Generators must evaluate each waste to determine if it's listed or exhibits a characteristic of hazardous waste (40 CFR 262.11). That evaluation must be made when the waste is first generated and must be documented. The challenge isn't the rule itself but how it applies to materials that fall between operational categories — products, wastes, and residuals.
Aerosols: When a common waste becomes a compliance risk
Aerosol cans are widely used across industries for maintenance, coatings, and cleaning. Facilities often assume that once a can is “empty” or depressurized, it's no longer subject to hazardous waste rules. That assumption can be risky.
If an aerosol can contains a listed solvent or exhibits ignitability (D001), it's a hazardous waste unless managed under an exclusion or alternative standard. Since 2019, many aerosol cans can be managed as universal waste (40 CFR Part 273), which simplifies handling. However, this option introduces its own requirements, including labeling, accumulation time limits, and proper puncturing practices.
A common issue arises at puncturing stations. For example, a maintenance shop installs a puncturing device and begins draining leftover propellant and product into a drum. The cans themselves may now meet the empty container standard, but the collected liquid often remains hazardous waste. In several inspections, regulators have cited facilities not for the cans, but for failing to characterize the accumulated liquid or for allowing it to evaporate without proper controls.
The lesson is straightforward: Shifting management methods (e.g., puncturing or using universal waste standards) doesn't eliminate the obligation to evaluate all resulting waste streams.
Residues: Small quantities, big implications
Residues are another frequent source of confusion. These can include paint booth sludge, tank bottoms, and material left in process equipment. Facilities sometimes view these materials as insignificant or assume they take on the classification of the original product. In reality, residues must be evaluated as newly generated wastes.
For example, a facility cleaning a parts washer may generate a sludge that contains spent solvent. Even if the waste solvent was originally a listed waste (e.g., F003 or F005), the generator must determine whether the residue is itself a listed waste or exhibits a characteristic. Missteps often occur when facilities rely on outdated Safety Data Sheets (SDSs) or assume that dilution or drying changes the classification.
Another scenario involves “letting residues dry out” in containers before disposal. While intended to reduce volume, this practice can be interpreted as treatment if it's done to change the waste’s characteristics (40 CFR 260.10 definition of treatment). For generators without a permit, this creates additional compliance risk.
The key takeaway is that residues aren't an afterthought. They are distinct waste streams that require their own evaluation and, in some cases, can trigger more stringent requirements than expected.
Empty containers: A rule often misapplied
The empty container rule (40 CFR 261.7) is widely cited but frequently misunderstood. A container that held hazardous waste is considered empty if all wastes have been removed using common practices (e.g., pouring, pumping), and no more than 1 inch of residue remains (or 3 percent by weight for smaller containers).
In practice, facilities often overapply this rule. For example, a drum that held a listed solvent may be declared empty even though significant sludge remains at the bottom. Inspectors routinely check this by tipping containers or visually assessing residue. If the container doesn't meet the standard, it's still subject to full hazardous waste requirements.
Another common issue involves containers that held acute hazardous waste (P-listed). These have stricter emptying standards, including triple rinsing. Facilities that overlook this distinction can inadvertently manage regulated containers as non-hazardous scrap.
Importantly, even when a container meets the empty standard, any removed residue must still be evaluated as a waste. The container may be exempt, but the material removed from it isn't.
Bringing it together in practice
Across these examples, a consistent pattern emerges: compliance issues arise when facilities rely on assumptions rather than applying the regulatory framework to each specific situation. Aerosols, residues, and empty containers all sit at the boundary between product use and waste management. That boundary is where most determination errors occur.
Facilities can reduce risk by standardizing evaluation procedures, training staff on common gray areas, and documenting determinations clearly. In inspections, regulators often focus less on the conclusion and more on whether the generator followed a defensible process under 40 CFR 262.11.
Key to remember: Every waste stream, no matter how small or routine, requires a fresh, documented determination at the point of generation. Management shortcuts don't replace regulatory obligations.

NewsHazardous WasteWaste GeneratorsWaste ManifestsWaste/HazWasteWasteEnvironmental Protection Agency (EPA)In-Depth ArticleUSAEnglishIndustry NewsWasteTSD FacilitiesWaste ManagementEnvironmentalFocus AreaWaste Reporting
2026-06-15T05:00:00Z
Hazardous waste manifest S Codes: What storage and transfer facilities need to know
Have you cracked the “S Code” yet? Starting in 2027, facilities that receive regulated waste for temporary storage and disposal must use S Codes on hazardous waste manifests. If your facility hasn’t made the switch, now’s the time!
Under the Resource Conservation and Recovery Act (RCRA), the Environmental Protection Agency (EPA) requires hazardous waste handlers to track shipments of regulated waste from the generating facility to final treatment, recycling, or disposal. Management Method Codes are key to hazardous waste manifests, and they also affect biennial reporting. The codes answer the vital question, “How’s the hazardous waste managed?"
Effective January 1, 2027, “S Codes” will officially replace Management MethodH141 for Storage and Transfer. EPA adopted these codes to improve the accuracy and transparency of waste tracking, specifically for wastes that travel through transfer facilities before final management. Use this overview to help your facility understand how to comply.
What are S Codes?
In January 2025, EPA added S Codes to the list of Management Method Codes, which identify the type of waste management system used to treat, recover, or dispose of a hazardous waste. Management Method Codes are used for:
- The Uniform Hazardous Waste Manifest (EPA Form 8700-22) and Continuation Sheet (EPA Form 8700-22A); and
- The National Biennial RCRA Hazardous Waste Report (EPA Form 8700-13 A/B), known as the Biennial Report.
S Codes apply to receiving facilities (primarily treatment, storage, and disposal facilities (TSDFs)) that temporarily store and then transfer regulated hazardous waste to another receiving facility without treating, recovering, or disposing of the waste. EPA established S Codes to provide more details than code H141 on waste handling activities, improving tracking and transparency. S Codes indicate two things:
- A hazardous waste was received to be stored or transferred; and
- The hazardous waste will be managed later by the final receiving facility using a certain method (i.e., the final management method).
EPA groups S Codes into three categories:
- Transfer off-site for reclamation and recovery,
- Transfer off-site for destruction or treatment prior to disposal, and
- Transfer off-site for disposal.
Each S Code corresponds to a specific final management method. Examples include metals recovery (S010), chemical treatment (S070), and landfilling (S132).
What’s required?
On January 1, 2027, EPA will remove Management Method Code H141 for Storage and Transfer from the e-Manifest and the Biennial Report forms. As a result, hazardous waste handlers must use S Codes instead of code H141 on manifests and the Biennial Report.
S Codes apply to RCRA hazardous waste that’s transferred off-site, impacting:
- Receiving facilities that store and transfer hazardous waste;
- Permitted TSDFs that receive hazardous waste solely for temporary storage and transfer (i.e., it’s the facility’s only management type); and
- Large quantity generators (LQGs) that report wastes shipped to transfer facilities on the Biennial Report.
Hazardous waste manifests
The first receiving TSDF is responsible for choosing and entering the S Codes on manifests. The storage and transfer facility must:
- Identify the S code that best describes how the hazardous waste will be managed by the final receiving facility, and
- Enter the S Code in Item 19 on the manifest and in Item 36 on the continuation sheet (if used).
Generators aren’t responsible for selecting or entering S Codes.
Biennial Reports
LQGs and TSDFs must use S Codes for the Biennial Report on the:
- Waste Generation and Management (GM) Form in Item 3, and
- Waste Received From Off-site (WR) Form in Item F.
LQGs use S Codes on the GM Form for shipments of hazardous waste off-site to a transfer facility for temporary storage and transfer.
TSDFs that receive hazardous waste for temporary storage and transfer off-site use S Codes on the WR Form. These TSDFs must also use Source Code G61 on the GM Form to report shipments of these transferred wastes.
How can facilities prepare?
Help your facility achieve a smooth shift to S Codes by January 1, 2027, with these tips:
- Identify where your facility currently uses code H141.
- Develop a process for transitioning to S Codes exclusively. Consider any changes your facility may need to make to its operations, such as updating software, adjusting procedures, and revising internal guidance documents.
- Train your employees accordingly.
- Set a deadline for making the switch to S Codes. Aim for a date well ahead of January 1, 2027, to give your facility enough time to address any issues that arise.
Key to remember: Starting in 2027, storage and transfer facilities must use S Codes in place of Management Method Code H141 on RCRA hazardous waste manifests and Biennial Reports.
NewsHazardous WasteWaste GeneratorsWaste ManifestsWaste/HazWasteWasteEnvironmental Protection Agency (EPA)In-Depth ArticleUSAEnglishIndustry NewsWasteTSD FacilitiesWaste ManagementEnvironmentalFocus AreaWaste Reporting
2026-06-15T05:00:00Z
Hazardous waste manifest S Codes: What storage and transfer facilities need to know
Have you cracked the “S Code” yet? Starting in 2027, facilities that receive regulated waste for temporary storage and disposal must use S Codes on hazardous waste manifests. If your facility hasn’t made the switch, now’s the time!
Under the Resource Conservation and Recovery Act (RCRA), the Environmental Protection Agency (EPA) requires hazardous waste handlers to track shipments of regulated waste from the generating facility to final treatment, recycling, or disposal. Management Method Codes are key to hazardous waste manifests, and they also affect biennial reporting. The codes answer the vital question, “How’s the hazardous waste managed?"
Effective January 1, 2027, “S Codes” will officially replace code H141 for Storage and Transfer. EPA adopted these codes to improve the accuracy and transparency of waste tracking, specifically for wastes that travel through transfer facilities before final management. Use this overview to help your facility understand how to comply.
What are S Codes?
In January 2025, EPA added S Codes to the list of Management Method Codes, which identify the type of waste management system used to treat, recover, or dispose of a hazardous waste. Management Method Codes are used for:
- The Uniform Hazardous Waste Manifest (EPA Form 8700-22) and Continuation Sheet (EPA Form 8700-22A); and
- The National Biennial RCRA Hazardous Waste Report (EPA Form 8700-13 A/B), known as the Biennial Report.
S Codes apply to receiving facilities (primarily treatment, storage, and disposal facilities (TSDFs)) that temporarily store and then transfer regulated hazardous waste to another receiving facility without treating, recovering, or disposing of the waste. EPA established S Codes to provide more details than code H141 on waste handling activities, improving tracking and transparency. S Codes indicate two things:
- A hazardous waste was received to be stored or transferred; and
- The hazardous waste will be managed later by the final receiving facility using a certain method (i.e., the final management method).
EPA groups S Codes into three categories:
- Transfer off-site for reclamation and recovery,
- Transfer off-site for destruction or treatment prior to disposal, and
- Transfer off-site for disposal.
Each S Code corresponds to a specific final management method. Examples of these methods include metals recovery (S010), chemical treatment (S070), and landfilling (S132).
What’s required?
On January 1, 2027, EPA will remove Management Method Code H141 for Storage and Transfer from the e-Manifest and the Biennial Report forms. As a result, hazardous waste handlers must use S Codes instead of code H141 on manifests and the Biennial Report.
S Codes apply to RCRA hazardous waste that’s transferred off-site, impacting:
- Receiving facilities that store and transfer hazardous waste;
- Permitted TSDFs that receive hazardous waste solely for temporary storage and transfer (i.e., it’s the facility’s only management type); and
- Large quantity generators (LQGs) that report wastes shipped to transfer facilities on the Biennial Report.
Hazardous waste manifests
The first receiving TSDF is responsible for choosing and entering the S Codes on manifests. The storage and transfer facility must:
- Identify the S code that best describes how the hazardous waste will be managed by the final receiving facility, and
- Enter the S Code in Item 19 on the manifest and in Item 36 on the continuation sheet (if used).
Generators aren’t responsible for selecting or entering S Codes.
Biennial Reports
LQGs and TSDFs must use S Codes for the Biennial Report on the:
- Waste Generation and Management (GM) Form in Item 3, and
- Waste Received From Off-site (WR) Form in Item F.
LQGs use S Codes on the GM Form for shipments of hazardous waste off-site to a transfer facility for temporary storage and transfer.
TSDFs that receive hazardous waste for temporary storage and transfer off-site use S Codes on the WR Form. These TSDFs must also use Source Code G61 on the GM Form to report shipments of these transferred wastes.
How can facilities prepare?
Help your facility achieve a smooth shift to S Codes by January 1, 2027, with these tips:
- Identify where your facility currently uses code H141.
- Develop a process for transitioning to S Codes exclusively. Consider any changes your facility may need to make to its operations, such as updating software, adjusting procedures, and revising internal guidance documents.
- Train your employees accordingly.
- Set a deadline for making the switch to S Codes. Aim for a date well ahead of January 1, 2027, to give your facility enough time to address any issues that arise.
Key to remember: Starting in 2027, storage and transfer facilities must use S Codes in place of code H141 on RCRA hazardous waste manifests and Biennial Reports.
New Network Poll


No active poll
Please come back soon!
Most Popular Highlights In Environmental

NewsHazmat SafetyIn-Depth ArticleUSASanitationWaste/HazWasteEnglishHR ManagementIndustry NewsFleet SafetySafety & HealthConstruction SafetyGeneral Industry SafetyAgriculture SafetyMaritime SafetySanitationRestroomsHandwashingEnvironmentalFocus AreaFleet OperationsMine SafetyTransportationHuman Resources
2023-04-06T05:00:00Z
Giving truck drivers rights to your restrooms
OSHA requires employers to provide all workers with immediately available and sanitary restroom or toilet facilities. But does this include truckers and delivery drivers that stop at your facilities? The sanitation standards (1910.141, 1926.51, and 1928.110) are meant to protect all workers from adverse health effects from unsanitary toilets facilities, or the unavailability of facilities when needed.
Proposed legislation
Bipartisan legislation has recently been introduced in the House that would require businesses to provide restroom access to truckers who are loading or delivering cargo at their warehouses, manufacturers, distribution centers, retailers, and ports.
Supported by leading organizations in the trucking industry, the Trucker Bathroom Access Act (H.R. 9592) was introduced on Dec. 15, 2022. The bill requires retailers, warehouses, and other establishments with existing restrooms to provide access to drivers who are loading or delivering cargo. Additionally, operators of ports and marine terminals must provide access for drayage and parking while accessing such restrooms.
This amendment to Title 49 would exempt some employers from the bill including filling and service stations, and restaurants 800-square feet or smaller with restrooms intended for employee use only. The bill doesn’t require employers to construct new restrooms but to give truck drivers the same access as employees or customers.
Your restroom availability affects their health
Commercial truckers and delivery drivers are the lifeline of our supply chain of supplies, products, and consumables. Working tirelessly all hours, during holidays and weekends, and throughout the pandemic, they continue to deliver critical food and emergency supplies to companies everywhere. Employers have the privilege of demonstrating gratitude to truckers and delivery drivers with a positive work environment.
The benefits of allowing truckers and delivery drivers the convenience and safety of readily available, sanitary restroom facilities are plenty. They’re able to rest and reset when necessary, which keeps them and others safer on the roads. Equally important, restroom availability prevents drivers from having to search for available facilities elsewhere, allowing them to keep a timely delivery schedule, limit supply chain delays, and ultimately lower costs for employers and customers.
Keys to remember
The proposed Trucker Bathroom Access Act will require retailers, warehouses, and other establishments with existing restrooms to provide access to truckers and delivery drivers who are loading or delivering cargo. Access to restrooms keeps them refreshed and ready to deliver essential supplies to companies across the country.

NewsIndustry NewsEnvironmental Protection Agency (EPA)CAA ComplianceEnvironmentalIn-Depth ArticleFocus AreaEnglishAir PermittingAir ProgramsAir ProgramsUSA
2025-05-23T05:00:00Z
Title V operating permits: Comply, certify, repeat
A Title V operating permit is a legally enforceable document with the federal and state air emissions regulations that a facility must meet to operate. One requirement that applies to all Title V permit holders is the annual compliance certification. It answers whether a facility fulfills the permit’s terms and conditions (such as emissions limits, monitoring, recordkeeping, and reporting).
Whether the Environmental Protection Agency (EPA) or a state or local regulatory agency issues the Title V permit, your facility must complete the annual compliance certification.
Discover what your facility needs to comply, certify, and repeat.
What’s required?
Facilities submit annual compliance certifications to the Title V permitting authority, which is usually a state or local regulatory agency (40 CFR 70.6). An EPA Regional Office serves as the permitting authority (71.6) for federally issued permits.
Title V tip: Check the state or local regulations for Title V compliance certification rules. They may require more frequent submissions and additional information.
At a minimum, the annual compliance certification covers two major areas for every permit term or condition:
- The compliance methods, and
- The compliance status.
Let’s take a closer look at each element.
Compliance methods
Your facility’s compliance methods are the ways it tracks whether it’s meeting the Title V permit requirements or not. When a term or condition isn’t met (like exceeding an emission limit), it’s known as a deviation.
Compliance methods consist of monitoring, recordkeeping, and reporting:
- Monitoring includes the procedures, test methods, and equipment used to track compliance data.
- Recordkeeping covers:
- The date, place, and time of monitoring;
- The date when monitoring results were analyzed, the entity that conducted the analysis, the analytical methods used, and the results; and
- The operating conditions during monitoring.
- Reporting consists of semiannual monitoring reports and deviation reports (which list the deviation, the applicable permit requirement, the probable cause, and any corrective or preventive actions).
Compliance status
Three questions determine the compliance status of each permit requirement during the covered period:
- Did the facility comply with the requirement?
- Was compliance continuous or intermittent?
- Were any deviations a “possible exception to compliance"?
Intermittent vs. continuous compliance
For each permit term or condition, your facility has intermittent compliance if it doesn’t meet the requirements at any time during the covered period. Your facility achieves continuous compliance only if it:
- Performs the necessary compliance methods,
- Has no unexcused deviations, and
- Records no contrary evidence.
Possible exception to compliance
EPA defines a possible exception to compliance as “any periods during which compliance is required and in which an excursion or exceedance … occurred” (70.6(c)(5)(iii)(C)).
Simply put, a possible exception to compliance is a deviation that occurs when compliance is mandated. If compliance isn’t required or another permit requirement excuses it, the deviation isn’t a possible exception.
How do I submit a compliance certification?
Your facility’s Title V permit provides instructions for how to submit the annual compliance certification, including the required forms and methods (via mail or electronic submission). You can also confirm requirements with your permitting authority. Generally, federally permitted facilities use the Annual Compliance Certification (EPA Form 5900-04).
Title V tip: Electronic submissions may be an option through the Compliance and Emissions Data Reporting Interface (CEDRI) on EPA’s Central Data Exchange. Check with your permitting authority to determine whether you may submit the annual compliance certification electronically via CEDRI.
Annual compliance certification is vital to maintaining your Title V permit. Keep in mind: comply, certify, and repeat.
Key to remember: Facilities with a Title V operating permit must certify compliance with the requirements at least annually.

NewsToxic Substances Control Act - EPAWasteWater ProgramsWater ProgramsCWA ComplianceEnglishAir ProgramsIndustry NewsIndustry NewsToxic Substances - EPAWasteAir ProgramsEnvironmentalFocus AreaUSA
2021-05-14T05:00:00Z
Enforcement Focus
A look at where regulators are focusing their enforcement efforts
Enforcement action and monetary penalties are unfortunately common in environmental programs and prove costly to companies. Beyond the penalty assessed, companies often spend even more improving processes to prevent recurrence. This section shares some of the headlines and presents take-away lessons. What happened and how do you avoid the same situation?
Air
Washington Department of Ecology issued a penalty to a pulp and paper mill in the state for air emissions released from the facility’s wastewater treatment plant. As the result of wastewater treatment plant upset conditions, the mill failed to meet emission reduction requirements for a seven-week period in 2020. The mill calculated an additional 7 tons of methanol and other types of hazardous air pollution were emitted from the operation during this period. In addition to the monetary penalty, the mill has been required to increase monitoring as a long-term preventative measure.
Enforcement action: $28,500 civil penalty
Lesson learned: A process upset in one part of an operation can have effects on related, but separate areas. Identifying and planning for these indirect impacts can reduce risk of noncompliance.
Hazardous waste
California’s Department of Toxic Substances Control (DTSC) reached a settlement with an electronic recycling facility in the state for hazardous and universal waste violations. Found during an inspection, DTSC identified multiple problems within the company’s waste management program. Violations included:
- Shredding of mercury-containing devices without a permit;
- Administrative issues including the lack of training, manifest deficiencies, improper emergency response procedures, and inadequate financial assurance;
- Storing of universal and hazardous wastes outside of designated areas and in excessive amounts; and
- Missing and inadequate labeling.
Enforcement action: $310,000 civil penalty
Lessons learned: Because of the serious health risks, mercury containing wastes require handling and disposal beyond those of other electronic wastes.
DTSC has taken a number of similar actions with other facilities in the state and appears to be making an extra push to hold sources accountable for potential and actual releases of toxic substances.
Water quality
The State of Illinois has entered settlement with a trucking distribution center related to an oil release that occurred in 2018. In 2018, the terminal released approximately 4,000 gallons of diesel fuel, from a leaking storage tank. The fuel entered the site drainage system, making its way to the nearby 4-acre pond, that then flows out into a local creek. The leak was not reported by the trucking terminal, escalating the severity of the incident. However, since the initial release the company has participated in cleanup plans and actions.
Enforcement action: $25,000 civil penalty
Lesson learned: Maintaining secondary containment, inspection programs, and level monitoring equipment are all best practices that can reduce risks of releases and associated costs.
Chemical reporting
U.S. EPA Region 5 announced settlement with a specialty chemical distributor for violations of the chemical data reporting (CDR) section of the federal Toxic Substances Control Act. The company failed to accurately report 18 chemicals that had been imported during the 2012 to 2015 compliance period. Chemicals distributed by the company are sold to a variety of manufacturing industries, that in turn use the substances in formulation of rubber, plastics, adhesives, sealants, and coatings.
Enforcement action: $357,000 civil penalty
Lesson learned: CDR reporting is an important source of data for EPA and something it takes seriously. Even though intermittent, these reports must be accurate and timely.
NewsHazardous WasteEnforcement and Audits - OSHAToxic Substances Control Act - EPAToxic Subtances Control Act - EPAElectronic Reporting of Injury and Illness RecordsTSCA ComplianceMonthly Roundup VideoCAA ComplianceUSAInjury and Illness RecordkeepingWaste/HazWasteEnglishOSHA Violations and PenaltiesIndustry NewsCrystalline SilicaWaste HandlersSafety & HealthGeneral Industry SafetyWasteWaste TransportersEnvironmentalFocus AreaToxic and Hazardous Substances - OSHAVideo
EHS Monthly Round Up - January 2025
In this January 2025 monthly roundup video, we'll review the most impactful environmental health and safety news.
Hi everyone! Welcome to the monthly news roundup video, where we’ll review the most impactful environmental health and safety news. There’s a lot going on, so let’s get started!
As happens at the start of most incoming presidential administrations, a freeze has been placed on all regulatory activity at the federal level, giving the new administration time to review agencies’ plans. The Office of Management and Budget, which must approve most rulemaking activities, has sent numerous pending rules back to the agencies for review. In addition, OSHA withdrew its infectious diseases proposed rule and its COVID-19 in healthcare rule prior to the inauguration.
OSHA’s penalties increased on January 15. The maximum penalty amounts for serious and other-than-serious violations increased to $16,550. For willful or repeated violations, the maximum penalty increased to $165,514 per violation.
OSHA updated its directive on injury and illness recordkeeping policies and procedures. While it’s intended for OSHA compliance officers, employers can use the information to help with recordkeeping compliance.
Fewer workers died on the job in 2023, as fatal work injuries decreased 3.7 percent from 2022. Transportation incidents remained the most frequent type of fatal event, accounting for over 36 percent of all occupational fatalities.
California’s Occupational Safety and Health Standards Board voted to adopt a permanent silica standard. If approved, it would extend and strengthen the state’s emergency temporary standard, which was put in place in December 2023.
The National Institute for Occupational Safety and Health updated its List of Hazardous Drugs in Healthcare Settings. This is a resource for employers and employees in identifying drugs that are hazardous to the health and safety of those who handle them.
Turning to environmental news, EPA released the biannual update of the nonconfidential TSCA inventory. The inventory helps facilities determine their regulatory requirements for the chemicals they use or plan to use.
And finally, EPA added new Management Method Codes to describe how hazardous waste will be managed after temporary storage and transfer. As of January 1st, hazardous waste handlers must use the codes on the Biennial Report Waste Generation and Management forms.
Thanks for tuning in to the monthly news roundup. We’ll see you next month!

NewsIndustry NewsWater PermittingWater ProgramsEnvironmental Protection Agency (EPA)Industrial WastewaterEnvironmentalIn-Depth ArticleCWA ComplianceEnglishFocus AreaUSA
2024-08-05T05:00:00Z
Industrial wastewater discharges: NPDES permits get to the point (source)
The Environmental Protection Agency (EPA) limits the pollutants in industrial wastewater that facilities can release through the National Pollutant Discharge Elimination System (NPDES) Program. Facilities require an NPDES permit to discharge pollutants directly into the waters of the United States.
Each permit lists the quantity, discharge rate, and concentration discharge limits for each pollutant (known as effluent limitations). The permit also covers monitoring and reporting requirements, applicable special conditions (like compliance schedules), and standard conditions that apply to all permits. States typically issue NPDES permits. EPA issues permits for just a handful of states and territories.
Does my facility require an NPDES permit?
The federal regulation at 40 CFR 122.1(b)(1) states that the NPDES program requires permits for the discharge of “pollutants” from any “point source” into “waters of the United States."
To determine whether your facility requires a permit, answer the following three questions.
Does the facility discharge covered pollutants?
The NPDES permit covers any kind of industrial, municipal, and agricultural waste that’s discharged into waters of the United States. It encompasses:
- Conventional pollutants, such as oil and grease;
- Nonconventional pollutants, like phosphorus; and
- Toxic pollutants, including solvents and metals.
EPA’s regulatory definition of “pollutants” (122.2) includes solid waste, sewage, chemical wastes, heat, rock, and more. However, it excludes sewage from vessels as well as certain materials injected into wells for oil or gas production and water derived from oil or gas production that’s disposed of in a well.
If your facility releases pollutants through its wastewater, the next factor to consider is how it discharges the pollutants.
Is the facility a point source?
A “point source” is defined at 122.2 as “any discernible, confined, and discrete conveyance … from which pollutants are or may be discharged.” It doesn’t include return flows from irrigated agriculture or agricultural stormwater runoff.
In clearer terms, a point source is a specific, identifiable source that discharges pollutants directly into a waterbody, like an industrial facility. Examples of points of discharge are pipes, ditches, tunnels, wells, and containers.
What if your facility discharges wastewater pollutants to a publicly owned treatment works facility? In this case, your facility is considered a non-point source (or indirect discharger) and must meet the requirements of the NPDES National Pretreatment Program.
Does the facility discharge into waters of the United States?
EPA’s current regulations define “waters of the United States” at 120.2. However, ongoing litigation has muddied the implementation of the current definition.
Here’s a general timeline of the definition’s changes:
- January 2023 — EPA and the Department of the Army updated the definition (Revised Definition of “Waters of the United States” rule).
- May 2023 — The U.S. Supreme Court’s decision in Sackett v. EPA (Case No. 21—454) made parts of the Revised Definition of “Waters of the United States” rule invalid.
- August 2023 — The agencies amended the Revised Definition of “Waters of the United States” rule to conform it to the Supreme Court’s decision. The final rule (Revised Definition of “Waters of the United States, Conforming” rule) took effect in September 2023.
Currently, EPA implements the definition according to the Revised Definition of “Waters of the United States, Conforming” rule in 23 states, the District of Columbia, and the U.S. territories. In the remaining 27 states, EPA implements the pre-2015 definition and interprets it consistently with the Sackett v. Environmental Protection Agency decision.
Make sure to confirm with your state’s wastewater permitting agency which definition of waters of the United States applies to your facility.
If you answer “yes” to all three questions, your facility must obtain an NPDES permit.
What’s next?
Now that you’ve determined your facility needs an NPDES permit, it’s time to apply for one:
- Connect with the state water permitting agency (or EPA if the state isn’t authorized to issue permits) to confirm that your facility requires a permit and determine what type of NPDES permit the state requires you to have (general or individual).
- Apply for the relevant NPDES permit through the permitting agency.
- Facilities under general permits typically submit a Notice of Intent to the permitting authority.
- Facilities not covered by general permits must apply for NPDES individual permits. Because these are developed for specific sites, the permitting process takes longer (possibly more than six months).
Key to remember: Facilities must obtain a general or individual NPDES permit before directly discharging industrial wastewater into waters of the United States.
NewsIndustry NewsEnvironmental Protection Agency (EPA)Oil Spill PreventionOil Spill PreventionEnvironmentalIn-Depth ArticleCWA ComplianceEnglishFocus AreaUSA
2026-06-30T05:00:00Z
Secondary containment alternative: Does your oil-filled operational equipment qualify?
Facilities that run like a well-oiled machine often rely on just that — operational equipment that stores and uses oil to function (like hydraulic systems). But wherever oil is stored, there’s always the possibility of a leak, and spilled oil can do serious harm, especially if it reaches water.
That’s where the Environmental Protection Agency’s (EPA’s) Spill Prevention, Control, and Countermeasure (SPCC) rule comes in. Usually, regulated facilities must equip oil-filled operational equipment with general secondary containment, which is designed to temporarily hold discharged oil until it can be properly cleaned up. However, some facilities may have another compliance option available.
EPA offers an alternative to secondary containment for qualified oil-filled operational equipment. Let’s take a look at the eligibility criteria and what the other method of compliance requires.
What’s oil-filled operational equipment?
EPA defines “oil-filled operational equipment” at 40 CFR 112.2. Generally, it refers to equipment that has one or more oil storage containers with oil that’s used solely to operate the equipment. Common examples are lubrication systems for pumps and compressors, machining coolant systems, circuit breakers, and electrical switches.
Does your facility have qualified equipment?
Only qualified oil-filled operational equipment is eligible for the alternative requirements to general secondary containment.
The SPCC rule considers oil-filled operational equipment to be qualified if it hasn’t had one discharge of oil exceeding 1,000 gallons or two discharges of oil exceeding 42 gallons each over the following time periods:
- If the facility has operated for at least 3 years, within any 12-month period in the 3 years before the SPCC Plan’s certification date; or
- If the facility has operated for less than 3 years, since becoming subject to the SPCC regulations.
Take note! When determining whether your facility’s oil-filled operational equipment is eligible under federal standards:
- Don’t count oil discharges caused by natural disasters, acts of war, or terrorism; and
- Don’t count the total amount of oil spilled, only the amount that reaches navigable waters or adjoining shorelines.
What about oil-filled manufacturing equipment?
The SPCC rule distinguishes between oil-filled manufacturing equipment and oil-filled operational equipment. Oil-filled manufacturing equipment stores oil only as a supporting element for conducting a mechanical or chemical operation to create or modify a product. It typically involves a flow-through process in which oil continuously moves through the equipment. Examples of this type of equipment include reaction vessels, mixing tanks, and distillation columns.
Because it’s defined independently under the SPCC rule, oil-filled manufacturing equipment isn’t eligible for the alternative compliance option available to qualified oil-filled operational equipment.
What are the alternative measures?
Instead of providing secondary containment for qualified oil-filled operational equipment, facilities may choose to comply with the alternative requirements at 112.7(k), which include:
- Establishing and documenting an inspection or a monitoring program to detect equipment failures and discharges; and
- Adding to the SPCC Plan:
- An oil spill contingency plan according to the requirements of Part 109; and
- A written commitment of the resources (manpower, equipment, and materials) needed to quickly control and remove any potentially harmful quantities of discharged oil;
Take note! If your business must submit a facility response plan (FRP) under 112.20, the oil spill contingency plan and written commitment requirements don’t apply since your FRP already contains these elements.
Why should my facility consider the alternative compliance option?
The alternative requirements to general secondary containment don’t require facilities to prepare an impracticability determination for qualified oil-filled operational equipment.
The impracticability determination provisions at 112.7(d) impose more requirements for facilities that use alternative measures to secondary containment for unqualified equipment.
In addition to meeting the same requirements for qualified oil-filled operational equipment, facilities must have the oil spill contingency plan certified by a Professional Engineer (unless self-certifying as a qualified facility). They also must:
- Describe in the SPCC Plan the reasons such measures aren’t practicable, and
- Conduct periodic integrity tests of bulk storage containers and periodic integrity and leak tests of valves and piping.
Key to remember: The SPCC rule offers an alternative to general secondary containment requirements for qualified oil-filled operational equipment.
Most Popular Highlights In Transportation

NewsIndustry NewsOn-duty time - Motor CarrierFleet SafetyHours of ServiceFocus AreaIn-Depth ArticleEnglishTransportationUSA
2023-08-16T05:00:00Z
Driver training time: On duty or off?
Training time is time spent wisely, but a big question remains: how should it be recorded?
Ongoing driver training is critical for ensuring that commercial motor vehicle drivers operate their vehicles safely and compliantly.
In fact, a recent report from the American Transportation Research Institute found that motor carriers who can access training materials and other resources from industry associations are safer than those who cannot. But is driver training time “on duty” or off?
It depends ...
Several variables will affect the answer:
- If a driver is required to go to a terminal or any other location for mandatory training, then the time must be recorded as “on duty.” That’s true whether the driver is paid or not. This falls under the category of “performing any ... work in the capacity, employ, or service of a motor carrier” under the definition of “on-duty time” in 49 CFR 395.2.
- If a driver has control over when and where the training is done, it’s done at the driver’s leisure, and it is not done during a period of time when the driver would otherwise have to be logging on duty (such as while waiting at a customer’s location), then it can be logged “off duty.”
- If a driver is off duty (such as at home for the weekend) but is given the training as a mandatory assignment and must complete it at a specific date, time, or location, then the training must be considered on-duty time.
| Get more insights about on-duty time in our ez Explanation! |
Nothing official
While federal regulations don’t address the issue directly, and the Federal Motor Carrier Safety Administration (FMCSA) has not issued any official word on it, there is some FMCSA guidance that touches on the issue:
Question: May the time a driver spends attending safety meetings, ceremonies, celebrations, or other company-sponsored safety events be recorded as off-duty time?
Guidance: Yes, if attendance is voluntary.
This guidance indicates that a driver may be performing a company-related activity without needing to record the time as on duty, as long as the driver has a choice to be there or not.
In addition, the following guidance refers to medical exams but could equally apply to training sessions:
Question: If a driver drives in a non-commercial vehicle to take a physical examination, should the duty status be recorded as on-duty not driving, or as off-duty? Would the answer change if the motor carrier directs the driver to go for the examination?
Guidance: So long as the driver schedules and attends the physical examination at a time of his or her own choosing, the time may be recorded as off-duty. If, however, the motor carrier directs the driver to attend at a specific time, the time is to be recorded as on-duty not driving.
Finally, it’s worth noting that if a driver is able to log off duty for a training session as discussed above, paying the driver for that time does not mean it has to be logged on duty:
Question: How does compensation relate to on-duty time?
Guidance: The fact that a driver is paid for a period of time does not always establish that the driver was on duty for the purposes of part 395 during that period of time. A driver may be relieved of duty under certain conditions and still be paid.
Key to remember: Driver training is highly recommended, but motor carriers often question how drivers should log the time. If certain conditions are met, training sessions can be logged off duty.

NewsIndustry NewsCarrier profiles, safety ratings and facility auditsSafety fitness certificatesWeights and dimensionsFleet SafetyLoad documentationFocus AreaIn-Depth ArticleEnglishSize and Weight LimitsOversize and Overweight MovementsTransportationUSA
2023-08-30T05:00:00Z
The Big and the Heavy: What you need to know about overweight trucks in Canada
Do you have questions on how to avoid or deal with driving an overweight truck in Canada? It can have serious consequences if your commercial vehicle is deemed overweight by the regulations of the jurisdiction where you plan to operate. When a vehicle is overweight, permits are issued for trucks and loads that exceed the weights set by the ruling transportation body of each province and permits are valid typically for highways only. If you want to drive on municipal roads, you may be required to get additional permits or permission directly from that municipality.
What you need to be aware of will depend on the province in which you are planning to operate. The maximum weight allowed for commercial vehicles in Canada depends on the registered gross vehicle weight (RGVW), the axle configuration and spacing, and the type of tires.
For example, in British Columbia, The maximum weight allowed for commercial vehicles in BC depends on the licensed gross vehicle weight (GVW), the gross combination vehicle weight (GCVW), the axle configuration and spacing, and the type of permit. The maximum GCVW for term permits in BC is 64,000 kg.
Checking your weight and dimensions
There are a few ways to estimate your vehicle’s weight. You can look up your vehicle by registration number or VIN or you can look in your vehicle’s manual or even call the manufacturer. The best way to get your vehicle’s weight is to weigh your vehicle using portable scales under each axle or by driving onto a scale. The rules, laws, and regulations for oversize in Canada are extensive and informative and are designed to ensure the safety of drivers, other road users, and the infrastructure.
The maximum legal limits allowed for height, width, and length are:
- Maximum width – 2.6 metres (vehicle and load)
- Maximum height – 4.15 metres (vehicle and load)
- Maximum length – 12.5 metres (single vehicle including load)
- Maximum length - 14.65 metres (semi-trailer including load)
- Maximum length (combination) - 23metres (combination vehicle and loads)
If your combination exceeds these dimensions, an oversize permit would be required.
Are you eligible for an overweight permit?
In Canada, whether or not you need an overweight permit for your trucks depends on the province you will be crossing and on many other different variables like axle spreads, specific axle weights, tire size, etc. This is why it is important to include as many details as possible when you fill out the application.
You are eligible to apply for a permit if your vehicle or load cannot be reduced because it:
- Could not be used for its intended purpose or function; and/or
- Would require more than eight work hours to dismantle.
You will not be eligible for a permit if your load is :
- Vehicle, load, or combination will be overweight, and your load is made up of more than one item;
- Vehicle or load is over height, over width, or overlength because of the way you have loaded it. For example, items are stacked in a way that creates unnecessary additional height, width, or length.
- Vehicle or load is overlength, your load is made up of more than one item, and the overhang of your load to the rear exceeds 4.65 metres from the centre of the rear-most axle
How do I get an oversize/overweight permit?
The process of getting a permit for an overweight truck may vary depending on the jurisdiction and the type of permit you need. You need to apply to the transportation authority of the province or territory where you plan to travel. The requirements, fees and conditions may vary depending on the type and size of your load and vehicle. You can find more information and online application forms on the websites of each province or territory.
The federal government does not issue permits for oversized or overweight vehicles.
How long is your permit valid?
Permits are good for a single trip meaning that if you cross from one province into the other and come back to your home province that permit is not valid anymore. For example, if you are based in Ontario, you deliver goods in Quebec and come back to Ontario, the permit you were issued is no longer valid. On the other hand, permits do have a validity period to complete your single trip and it can range from 48 hours to 10 days depending on which province the permit was issued in. Always read your permit to ensure you’re complying with its conditions.
Key to remember: To avoid overweight issues, plan your route to avoid roads or bridges that have weight restrictions, make sure your load is evenly distributed, obtain the proper permits, and most importantly follow the safety standards and regulations in your jurisdiction.

NewsPersonal Protective EquipmentTransportationIn-Depth ArticleEnglishWork ZonesIndustry NewsSafety VestsFleet SafetySafety & HealthConstruction SafetyGeneral Industry SafetyMaritime SafetyWork ZonesFlaggersFocus AreaUSA
2024-02-20T06:00:00Z
Safety vests: MUTCD overhaul rule shakes up mandates
The Federal Highway Administration (FHWA) finalized sweeping revisions for the 11th edition of the Manual on Uniform Traffic Control Devices for Streets and Highways (MUTCD). Last updated in 2009, the MUTCD is the national standard for traffic signs, signals, and markings, including work zones. Changes took effect January 18.
Section 6C.05 (previously Section 6E.02), is entitled, “High-Visibility Safety Apparel.” It’s noteworthy that FHWA revises that section to replace the reference to the 2004 edition of ANSI/ISEA 107, American National Standard for High-Visibility Safety Apparel and Headwear,” with the 2015 edition.
What about OSHA?
OSHA work zone mandates are short on text, but they're found in 29 CFR 1926 Subpart G, Signs, Signals, and Barricades. The OSHA regulations specifically say:
- 1926.200(g) Traffic control signs and devices. (1) At points of hazard, construction areas shall be posted with legible traffic control signs and protected by traffic control devices. (2) The design and use of all traffic control devices, including signs, signals, markings, barricades, and other devices, for protection of construction workers shall conform to Part 6 of the MUTCD (incorporated by reference, see § 1926.6).
- 1926.201(a) Flaggers. Signaling by flaggers and the use of flaggers, including warning garments worn by flaggers, shall conform to Part 6 of the MUTCD (incorporated by reference, see § 1926.6).
How do OSHA and FHWA relate?
OSHA’s mission is to protect workers. FHWA, an arm of the DOT, aims to protect motorists/pedestrians. Yet, FHWA also provides protection for road workers under:
- 23 CFR 630, Subpart J, Work Zone Safety and Mobility;
- 23 CFR 630 Subpart K, Temporary Traffic Control Devices; and
- 23 CFR 655, Subpart F, Traffic Control Devices on Federal-Aid and Other Streets and Highways.
Both OSHA and DOT refer to the MUTCD for traffic control of work zones. However, the two agencies refer to different editions of the manual:
- FHWA 23 CFR 630 and 655 refer to the MUTCD, December 2023 edition; and
- OSHA 1926.200 and .201 refer only to Part 6 of the MUTCD, December 2009 edition (including Revisions 1 and 2, May 2012).
High-visibility safety apparel and FHWA
FHWA and Section 6C.05 of the 2023 MUTCD require all workers to wear high-visibility safety apparel if they are in the right-of-way and within a “temporary traffic control” (TTC) zone. This includes flaggers and emergency responders, night or day. The apparel must meet Performance Class 2 or 3 requirements of ANSI/ISEA 107-2015. The only exception is for emergency/incident responders and law enforcement in the TTC zone. In those cases, they may wear apparel that meets ANSI/ISEA 207-2006, American National Standard for High-Visibility Public Safety Vests.
In all cases, the apparel background material color must be fluorescent orange-red, fluorescent yellow-green, or a combination of the two. The retroreflective material must be orange, yellow, white, silver, yellow-green, or a fluorescent version of these colors.
High-visibility safety apparel and OSHA
OSHA still adheres to the 2009 MUTCD as revised in 2012. Section 6E.01 requires flaggers to wear high-visibility safety apparel that meets Performance Class 2 or 3 requirements of ANSI/ISEA 107-2004.
The OSHA-adopted MUTCD calls for the apparel background material color to be fluorescent orange-red, fluorescent yellow-green, or a combination of the two. The retroreflective material must be visible from at least 1,000 feet and be orange, yellow, white, silver, yellow-green, or a fluorescent version of these colors. Moreover, the apparel must clearly identify the wearer as a person.
OSHA’s de minimis policy
When both FHWA and OSHA regulations apply, which MUTCD and ANSI standard do you follow? The answer may be found in a May 11, 2004, OSHA letter of interpretation. The letter explains, “Under OSHA's de minimis policy, compliance with more current DOT requirements, or with more current ANSI or other applicable nationally recognized consensus standards, is acceptable, so long as such standards are at least as protective as the OSHA requirement.”
Under OSHA's de minimis policy, the violations have no direct or immediate relationship to safety or health, so they are considered de minimis. De minimis violations of standards exist when you comply with the clear intent of the standard but deviate from its particular requirements, and there’s no direct or immediate impact on the safety and health of workers. OSHA says it does not impose penalties or require correction of de minimis violations.
The letter adds that high-visibility apparel is required not only under 29 CFR 1926 Subpart G but also Section 5(a)(1) of the OSH Act (General Duty Clause) to protect employees exposed to traffic hazards while working in road construction work zones.
Key to remember
FHWA revised the MUTCD, including high-visibility apparel requirements. OSHA’s regulations have not changed, but where FHWA and OSHA both apply, employers may turn to OSHA’s de minimis policy.

NewsIndustry NewsFleet SafetyElectronic logging device (ELD)Electronic logging device (ELD)Fines and penalties - Motor CarrierEnforcement - DOTFocus AreaIn-Depth ArticleEnglishTransportationUSA
2023-10-04T05:00:00Z
Company gets $50,000 lesson in ELD mounting rules
A truck driver who knew the rules for mounting his electronic logging device (ELD) better than his employer did was awarded nearly $50,000 in damages after he blew the whistle.
The driver was given a portable ELD but no mount. He refused to drive the vehicle, citing federal regulations that require portable ELD displays, such as phones or tablets, to be mounted in the cab.
Gross insubordination
The company, a major nationwide freight hauler, tried to coerce him into driving and then terminated him for “gross insubordination.” The company later reinstated him and changed his termination to a suspension, but then continued to harass him, according to the Occupational Safety and Health Administration (OSHA).
The driver filed a whistleblower complaint with OSHA and won the case. His employer was forced to pay him $15,273 in compensatory damages, $30,000 in punitive damages, and approximately $2,700 in back wages plus interest.
Know the rules!
The case serves a reminder that employers violate federal law if they fire, suspend, or otherwise retaliate against any driver who refuses in good faith to violate the Federal Motor Carrier Safety Regulations.
In this case, the FMCSA regulations in 395.22(g) are clear:
“If a driver uses a portable ELD, the motor carrier shall ensure that the ELD is mounted in a fixed position during the operation of the commercial motor vehicle and visible to the driver when the driver is seated in the normal driving position.”
A related provision discusses the potential need to unmount the display and hand it outside the vehicle:
“An ELD must be designed so that its display may be reasonably viewed by an authorized safety official without entering the commercial motor vehicle. For example, the display may be untethered from its mount or connected in a manner that would allow it to be passed outside of the vehicle for a reasonable distance.”
No matter the rule, if a driver refuses to drive due to a safety regulation, be sure to study the regulation and verify the driver’s claim before rushing to judgment. Taking the time to know the rules and educate your drivers could save time, money, and headaches in the long run.
Key to remember: Coercing a driver to operate a commercial vehicle despite his or her argument that it would violate a safety regulation can be illegal and result in hefty fines.

NewsIndustry NewsFleet SafetyDriver qualificationsDrivers qualification (DQ file)Driver qualification and hiringEmployment application driverIn-Depth ArticleFleet OperationsFocus AreaEnglishTransportationUSA
2026-03-25T05:00:00Z
The non-domiciled CDL final rule: A compliance reality check
On March 16, 2026, the Federal Motor Carrier Safety Administration (FMCSA) implemented a sweeping final rule aimed at fundamentally changing how non domiciled Commercial Driver’s Licenses (CDLs) are issued in the United States. Officially titled “Restoring Integrity to the Issuance of Non Domiciled Commercial Driver’s Licenses,” the rule amends 49 CFR Parts 383 and 384.
The rule establishes strict eligibility standards, imposes new verification requirements on states, and is backed by aggressive enforcement expectations that extend beyond licensing offices to roadside inspections and carrier audits.
What the final rule requires
The final rule sharply limits eligibility for non domiciled CDLs and Commercial Learner’s Permits (CLPs). Under the new regulation, only three immigration categories qualify:
- H 2A – Temporary agricultural workers
- H 2B – Temporary non agricultural workers
- E 2 – Treaty investors and qualifying employees
No other immigration status, regardless of employment authorization, may be used to obtain, renew, transfer, or upgrade a non domiciled CDL or CLP.
A key requirement of the rule is mandatory immigration status verification. State Driver Licensing Agencies (SDLAs) must verify a driver’s lawful status through the federal SAVE system and may not rely on Employment Authorization Documents (EADs), or pending immigration applications as proof of eligibility. If a state cannot meet these verification standards, it is required to halt issuance of all non domiciled CDLs and CLPs until compliance is achieved.
The rule also restricts the validity period of non domiciled CDLs. Licenses may not exceed one year or extend beyond the expiration date of the driver’s lawful immigration status, whichever comes first. Each renewal requires fresh verification under the same standards.
Who the rule affects
The rule directly affects foreign domiciled drivers who operate commercial motor vehicles in the United States under non resident CDLs. FMCSA estimates that approximately 190,000–200,000 drivers could lose eligibility over time due to non renewals or license revocations. Drivers previously relying on broader categories are no longer eligible under the final rule. Motor carriers are also affected. FMCSA guidance makes clear that carriers employing drivers whose licenses later become invalid face increased exposure during driver qualification audits, investigations, and enforcement actions. The rule reinforces that responsibility for compliance extends beyond the driver to the employer. Importantly, the rule does not apply to U.S. citizens, lawful permanent residents, or drivers licensed in Canada or Mexico who operate under existing reciprocity agreements.
Why FMCSA Implemented the Rule
FMCSA found widespread state non compliance and systemic weaknesses in the verification of foreign driving histories as the primary reasons for the rule. According to the agency, a nationwide review found that more than 30 states had issued tens of thousands of non domiciled CDLs using standards that did not meet existing federal requirements.
Safety concerns were central to the decision. FMCSA documented 17 fatal crashes in 2025 resulting in 30 deaths involving non domiciled CDL holders who would not have been eligible under the new rule. While acknowledging that these crashes represent a small fraction of overall CMV fatalities, FMCSA stated they illustrate the potential risks created when driver history, status, and qualification cannot be reliably verified.
The agency framed the rule as necessary to restore integrity, uniformity, and accountability to the CDL system while closing gaps that allowed improperly issued licenses to remain in circulation.
Key to Remember: The Non Domiciled CDL Final Rule represents a decisive shift from flexibility to strict federal oversight. It narrows eligibility, mandates verification, shortens license duration, and places renewed emphasis on carrier responsibility.
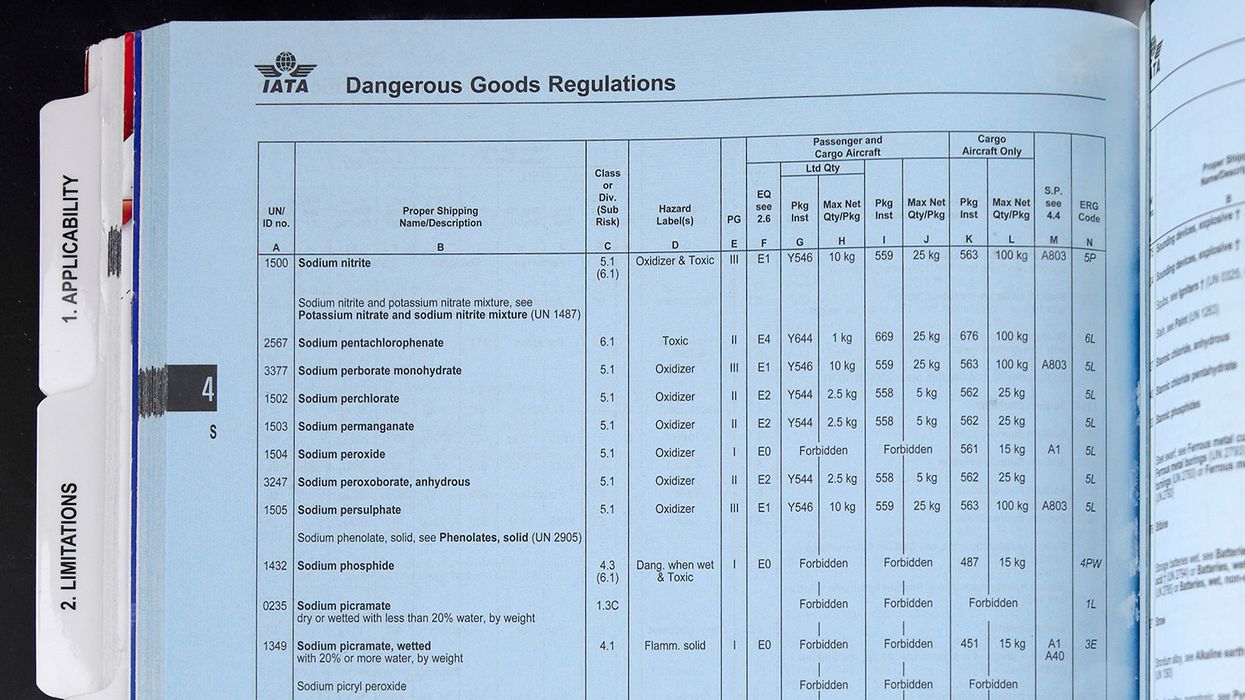
NewsIndustry NewsHazmat SafetyHazmatIn-Depth ArticleFocus AreaUSAEnglishTransportationHazmat Rulemaking procedures
2023-12-22T06:00:00Z
Navigating change: Key updates to 2024 IATA DGR take effect
Every year the International Air Transport Association (IATA) updates its Dangerous Goods Regulations (DGR) to ensure the safe and secure handling of dangerous goods that are shipped or transported by air. While changes to the 2024 IATA DGR (65th edition) are not as plentiful as they were in previous years, they are no less important.
Mandatory compliance with the 2024 IATA DGR begins on January 1, 2024, and will be valid until the 2025 IATA DGR comes into effect. Let’s look at the key updates, listed by Section, for the 65th edition of the IATA DGR:
Need additional information for IATA? Check out this ezExplanation.
Limitations
- Dangerous Goods Carried by Passengers or Crew (2.3)— Provisions for battery-powered mobility aids have been revised to include reference to the guidance on the end-to-end processes associated with the carriage of mobility aids.
Packing
The following packing instructions have been updated:
- 5.2.0.9 - Added a water capacity limit for non-refillable cylinders containing a flammable gas, limited to a water capacity not exceeding 1.25 L.
- PI 952 - Revised to include reference to "equipment."
- PI 954 - Clarified the rules for marking overpacks containing dry ice. The total net quantity of dry ice in the overpack must be marked on the outside of the overpack.
Packaging specifications and performance tests
- 6.0.3 - Clarified the requirements and formatting for UN specification marks on packages.
Documentation
- 8.1.6.9.2, Step 6 – Added a note to "reinforce that there is no requirement for the type, number and net quantity in inner packagings within the outer packaging of a combination packaging to be shown" on the shipping papers (Shippers Declaration for Dangerous Goods).
Radioactive materials
- 10.8.3.9.1—Added an additional example of the description for the first sequence of information on the Shipper's Declaration to address where a radioactive material has a subsidiary hazard, and the proper shipping name must be supplemented by the technical or chemical name.
- 10.8.6—Added two examples to show how radioactive materials with a subsidiary hazard should be described and how packages in an overpack should be shown.
Appendices
IATA has added a new appendix to the list of appendices in the DGR. Appendix H includes a list of changes IATA will make to the 2025 IATA DGR. IATA added Appendix H so that shippers and carriers have time to prepare for the substantial updates that are coming for 2025. Some of the changes include:
- Adding an exception for data loggers and cargo trackers with installed lithium batteries.
- Modifying the exception for COVID-19 vaccines to now apply to all pharmaceutical products.
- Adding a new classification for sodium ion batteries.
- Updating the list of dangerous goods and special provisions.
- Amending and adding several packing instructions.
- Revising the "lithium battery mark", which will be known as the "battery mark" in the future.
Making sure you are keeping up with these regulatory changes and preparing for future updates is extremely important if you want to avoid costly delays, fines, and lost revenue. Keep your hazmat employees up to speed and inform them of any changes they need to be aware of.
Key to Remember: IATA updates their DGR every year and changes to the 2024 IATA DGR become effective on January 1, 2024.
Most Popular Highlights In Human Resources

NewsIndustry NewsIndustry NewsHR GeneralistFamily and Medical Leave Act (FMLA)Family and Medical Leave Act (FMLA)USAHR ManagementEnglishFocus AreaHuman Resources
2023-09-06T05:00:00Z
Appellate court sided with employee's (almost) 3-year-delayed FMLA claim
Back in October 2018, Laffon had a medical emergency and needed some time off under the federal Family and Medical Leave Act (FMLA).
Her leave lasted until November 15. Ten days after she returned to work, on November 26, her employer terminated her.
She sued, arguing that the employer retaliated against her because of her FMLA leave.
The catch? She didn't bring the suit until almost three years later.
No link between leave and termination
In court, the employer argued that there was no causal link between Laffon taking FMLA leave and her termination. Although the court documents aren't robust, they do reveal that the employer indicated that Laffon's allegations didn't show that her taking FMLA leave was a factor in the decision to terminate her. The documents showed only that the termination chronologically followed her leave.
The court agreed with the employer. It also agreed that Laffon failed to allege a willful violation of the FMLA, which would allow her to benefit from the FMLA's three-year statute of limitations.
Laffon appealed the case to the Ninth Circuit.
Statute of limitations
Under the FMLA, employees have two years from the date of the last event constituting the alleged violation for which they can bring a claim.
Those two years are extended to three years if the employer's actions were "willful." This means that an employee must show that the employer either knew or showed reckless disregard for whether its conduct violated the FMLA.
Ruling overturned
Fast forward to August 2023, when the Ninth Circuit reversed the lower court's decision. It indicated that, based on Laffon's amended complaint and liberally construing the law, her allegations establish that her leave was causally connected to her termination and that the employer's action (her termination) was willful.
Glymph v. CT Corporation Systems, No. 22-35735, Ninth Circuit Court of Appeals, August 22, 2023.
Key to remember: Terminating an employee soon after returning from FMLA leave is risky, unless there is a clear, well-documented, non-leave-related reason. Case documents did not show such a clear reason, which can also increase the risk of a willful finding. Employees have time to file claims, even years.

NewsIndustry NewsHR GeneralistFamily and Medical Leave Act (FMLA)In-Depth ArticleFamily and Medical Leave Act (FMLA)HR ManagementEnglishUSAFocus AreaHuman Resources
2026-06-23T05:00:00Z
Elective procedures and the FMLA
With employees being more open to obtaining elective medical procedures again, employers might see an increase in employees asking for time off for them. Employees might be entitled to job-protected leave under the federal Family and Medical Leave Act (FMLA) for such procedures. Just because a procedure is deemed “elective” doesn’t always matter.
What the FMLA regulations say
Employers might think that the FMLA regulations say that employees don’t get FMLA leave for elective procedures. The regulations, however, make it clear that, in some situations, employees may, and that just because a procedure is elective doesn’t automatically mean it’s not FMLA-qualifying.
“Conditions for which cosmetic treatments are administered (such as most treatments for acne or plastic surgery) aren’t serious health conditions unless inpatient hospital care is required or unless complications develop.” [29 CFR 825.113(d)]
The word “unless” means that there are exceptions.
Therefore, if an employee has an overnight stay in a health care facility, whether the procedure is elective or not, it won’t matter; it’s an FMLA-qualifying serious health condition. If, for example, a perfectly healthy employee decides to donate a kidney to a sibling, the time off for the procedure and recovery from it will fall under the FMLA, as the employee will be kept overnight in the hospital — it will be an inpatient situation.
Another example would include a situation in which an employee’s procedure results in a period of incapacity for more than 3 consecutive calendar days, and any subsequent treatment that also involves:
- Treatment two or more times, within 30 days of the first day of incapacity, unless extenuating circumstances exist, or
- Treatment by a health care provider on at least one occasion, which results in a regimen of continuing treatment under the supervision of the health care provider.
Some of the more common elective procedures employers might have employees ask for time off include:
- Hysterectomy
- Liposuction
- Breast reduction/augmentation
- Joint replacement
- Facelift
- Rhinoplasty
- Cataract removal
- Tonsillectomy
Some elective procedures are designed to improve the quality of life as opposed to saving lives in emergencies.
Employers shouldn’t focus on the name of the condition or procedure, but on whether the condition meets the FMLA’s definition of a serious health condition, which is on the last page of the certification.
When employees ask for time off for what might be an FMLA-qualifying reason, employers should treat the situation as they would any FMLA leave request, including asking for a certification supporting the need for leave. It should give employers enough information to determine if the condition meets the FMLA’s definition of a serious health condition.
Key to remember: Employees could be entitled to FMLA leave for elective medical procedures, depending on all the facts involved.

NewsIndustry NewsPerformance ManagementAssociate Benefits & CompensationHR GeneralistFamily and Medical Leave Act (FMLA)Focus AreaIn-Depth ArticleFamily and Medical Leave Act (FMLA)Performance AppraisalsEnglishHR ManagementAssociate RelationsHuman ResourcesUSA
2023-01-12T06:00:00Z
Performance review timing and FMLA leave
A new year often begins a new round of employee performance reviews. Since the Family and Medical Leave Act (FMLA) allows eligible employees to take up to 12 (or 26) weeks of leave, many events can occur during an employee’s leave, including the employee’s pre-scheduled performance review. Such reviews might take place on an annual or other scheduled basis. How you treat the timing of those reviews should include some thought.
If, for example, Jo Employee takes 12 weeks of FMLA leave, during which her annual performance review is scheduled, here are some questions to ponder:
- Do you look at all 12 months of Jo’s performance?
- What if she hasn’t worked a full 12 months because of leave?
- When can you actual do the review?
- Can you delay it so you can look at a full 12-months of work?
Delaying a review
An annual performance review generally takes into consideration a full years’ worth of work. Some employers think it’s best to delay the performance review by the same amount of time an employee took FMLA leave to capture an entire years’ work. This practice, however, might risk running afoul of one of the cornerstones of the FMLA: Returning the employee to his or her position, including the equivalent pay, benefits, and working conditions.
The issues can be particularly concerning if the performance review affects wage increases or other compensation.
What the regulations say
The FMLA regulations indicate that an equivalent position includes equivalent pay, which includes any unconditional pay increases that may have occurred during the FMLA leave period. Equivalent pay also includes bonuses or payments, whether discretionary or non-discretionary. FMLA leave cannot undermine the employee’s right to such pay.
Furthermore, “… employers cannot use the taking of FMLA leave as a negative factor in employment actions, such as hiring, promotions, or disciplinary actions; nor can FMLA leave be counted under no fault attendance policies.” [29 CFR 825.220(c)]
Avoiding a negative factor
Therefore, you would need to look at whether delaying an employee’s performance review could be seen as having a negative factor for the employee.
If, for example, Jo Employee took 12 weeks of leave from April through June, during which she would otherwise have obtained a pay increase in May, but you delayed this increase until September (so you could use a full 12 months of work), you may have violated the equivalent pay provision. If delaying a review creates a new review schedule going forward, the negative impacts could continue.
If, however, a pay increase is conditioned upon seniority, length of service, or work performed, you would grant it in accordance with your policy or practice as applied to other employees on an equivalent leave status for a reason that does not qualify as FMLA leave.
In other words, don’t treat an employee on FMLA leave differently than you would an employee on other forms of leave.
Key to remember: It might be less risky to keep the performance review on schedule and prorate wage increases to account for FMLA leave.

NewsIndustry NewsHR GeneralistFamily and Medical Leave Act (FMLA)In-Depth ArticleFamily and Medical Leave Act (FMLA)HR ManagementEnglishUSAFocus AreaHuman Resources
2023-09-07T05:00:00Z
Did you know? Part-time employees may take FMLA leave
Private employers with 50 or more employees in the U.S. and all public employers must provide leave under the federal Family and Medical Leave Act (FMLA) to employees who meet certain eligibility criteria.
Those employees, however, don’t need to work full-time schedules to qualify for FMLA.
Whether an employee is part-time, full-time, seasonal, and so on does not affect their FMLA eligibility.
Employee eligibility
To be eligible to take FMLA leave, employees must meet all three of the following criteria:
- Work for the company for at least 12 months (need not be continuous),
- Worked at least 1,250 hours in the 12 months before leave is to begin, and
- Work at a location with at least 50 company employees within 75 miles.
Employees who work a little more than 26 hours per week will meet the 1,250 hours worked threshold. Therefore, simply indicating that part-time employees are not eligible for FMLA leave would risk a violation of the law.
Seasonal employees, for example, who work about 52 hours per week for six months will also meet the 1,250 hours worked threshold.
Some part-time or seasonal employees will not meet all the eligibility criteria because of their limited months or hours worked. In that case, they would not be eligible to take FMLA leave.
How much FMLA leave
Part-time employees may take 12 of their workweeks of FMLA leave in a 12-month leave year period. The hourly equivalent of those 12 workweeks depends on what an employee’s schedule looks like.
An employee works 30 hours per week will have 360 hours of FMLA leave. In contrast, an employee who normally works 50 hours per week will have 600 hours of FMLA leave. The number of hours in an employee’s FMLA leave “bucket” only really comes into play for intermittent leave. Otherwise, a workweek is a workweek regardless of how many hours an employee typically works.
If an employee who works 30 hours per week begins five weeks of leave on Monday, September 11, he would return to his 30-hours per week schedule on Monday, October 16.
Tracking intermittent leave
When employees take leave intermittently or on a reduced schedule, tracking the leave can be more challenging.
To determine how many hours of FMLA leave the employee as available, employers simply multiply the number of hours an employee works in a workweek by 12.
Many part-time employees work variable hours each week. Sometimes an employee’s schedule varies so much that an employer can’t determine how many hours the employee would have worked before taking FMLA leave.
In that situation, the employer should use a weekly average of the hours worked over the 12 months before leave begins to calculate how many hours of FMLA leave the employee has available.
Key to remember: Part-time employees can be eligible to take 12 weeks of FMLA leave, but they need to meet certain criteria. How many hours intermittent or reduced schedule FMLA leave employees may take depends upon how many hours they work per week.

NewsIndustry NewsRecordkeepingRecordkeepingHR GeneralistFamily and Medical Leave Act (FMLA)In-Depth ArticleFamily and Medical Leave Act (FMLA)HR ManagementEnglishUSAFocus AreaHuman Resources
2026-05-20T05:00:00Z
Do the FMLA notices and certifications expire in June?
The answer to that question for employers is, “No.” The answer to that question for the U.S. Government’s Office of Management and Budget (OMB), however, is, “Yes.”
Employers might notice that the following federal Family and Medical Leave Act (FMLA) documents from the U.S. Department of Labor (DOL) have an expiration date listed as “6/30/26” in the upper right-hand corner:
- WH-381: Eligibility/Rights and Responsibilities Notice
- WH-382: Designation notice
- WH-380-E: Certification of an employee’s serious health condition
- WH-380-F: Certification of a family member’s serious health condition
- WH-384: Certification of a qualifying exigency
- WH-385: Certification for military caregiver of a current military member
- WH-385-V: Certification for military caregiver of a veteran
This, however, doesn’t mean that employers aren’t allowed to use these forms after that date. They may. Employers and employees are allowed to use the current forms beyond that date because the content remains applicable under FMLA law.
The June 30, 2026, date on the FMLA notices and certification forms, doesn’t represent a deadline for FMLA leave itself. It’s the OMB’s expiration date for the forms’ collection and recordkeeping requirements, not the end of the forms’ legal validity.
What the date means
These government documents are subject to certain checks and balances, such as the following:
- OMB control number 1235‑0003 governs the collection of information from employers and employees for DOL compliance purposes.
- The June 30, 2026, date is when the latest version of the forms will be replaced by a new OMB‑approved version.
The OMB has to review the FMLA notices and certification forms every 3 years. The last time it did so, it didn’t make any material changes.
The OMB is part of the U.S. Executive Office and helps the president meet policy and budget, manage details, oversee regulatory objectives, and helps fulfill the agency’s statutory responsibilities.
Model forms optional
Employers aren’t required to use the DOL’s model forms. Many do, however, because it’s easier than creating their own forms. Using the DOL’s forms also helps ensure the notices provide enough information and the certifications don’t ask employees for information beyond what the FMLA allows.
Key to remember: The June 30, 2026, expiration date of FMLA documents is just a form‑collection deadline, not a legal cutoff for FMLA leave or certification. Employers may still use the current forms until a new version is issued.

NewsIndustry NewsHR GeneralistFamily and Medical Leave Act (FMLA)In-Depth ArticleFamily and Medical Leave Act (FMLA)Associate RelationsEnglishUSAHR ManagementFocus AreaHuman Resources
2022-12-14T06:00:00Z
Must employers tell employees if they run out of FMLA?
There’s a lot to keep track of when administering employees’ time off, especially when it falls under the Family and Medical Leave Act (FMLA).
Employers might wonder if they need to tell employees when their FMLA leave is running out. And the simple answer is “not really.”
Neither the statute nor the regulations specifically require you to notify or remind employees that their FMLA leave exhausted or is close to it. If you know how much time FMLA leave an employee is taking, you are, however, required to include that information on the designation notice. But, otherwise, there isn’t any other form or required document to tell an employee, “Hey, you’re running low on FMLA leave.”
Does this mean you may not give employees such a reminder?
Again, the simple answer is “no.” Employers may even have good arguments for doing so.
Why a gentle reminder can be helpful
When employees are on FMLA leave, the reason behind the need for leave will probably be of great importance to the employee. It could be because a baby was born or because a family member has a serious health condition. In any case, the employees most likely have a lot on their mind. They might not be constantly thinking about when they will return to work or when they will run out of FMLA leave.
Providing a gentle reminder can show employees that you’re thinking of them, and that you expect them to return on a particular date. Employees generally appreciate knowing what is expected of them. Giving them such a reminder can also help allay any questions about whether they knew they were expected back on such a date.
This could also be a good opportunity to remind employees that if they cannot return to work because of continued issues with their own serious health condition, they should let the employer know. In cases like this, an employer then can engage in an interactive process (dialogue) with the employee regarding possible reasonable accommodations under the Americans with Disabilities Act. One accommodation, for example, might be more leave time.
Providing employees with reminders about how much leave time they have left can also address the consequences for any absences after FMLA protections expire. This is especially important in terms of maintaining employee benefits.
Designation notice changes
If the information in the designation notice changes, such as if the employee exhausts FMLA leave then requests more leave, you must provide a written notice of the change. Like with the original designation notice, a change notice must be given to the employee within five business days of receipt of the employee’s first notice of need for additional leave.
Therefore, if, after an employee exhausts all 12 weeks of FMLA leave, the employee asks for more leave, you are to notify the employee of the changes to the designation notice. You may use another designation notice if you wish, but you are not required to do so. You could simply indicate to the employee that there is no more FMLA leave available, so the additional leave will not be designated as FMLA leave.
Key to remember: Keeping the lines of communication open between you and employees who are on FMLA leave can benefit both employers and employees, even if all types of communication aren’t necessarily required.
Most Popular Highlights In Safety & Health
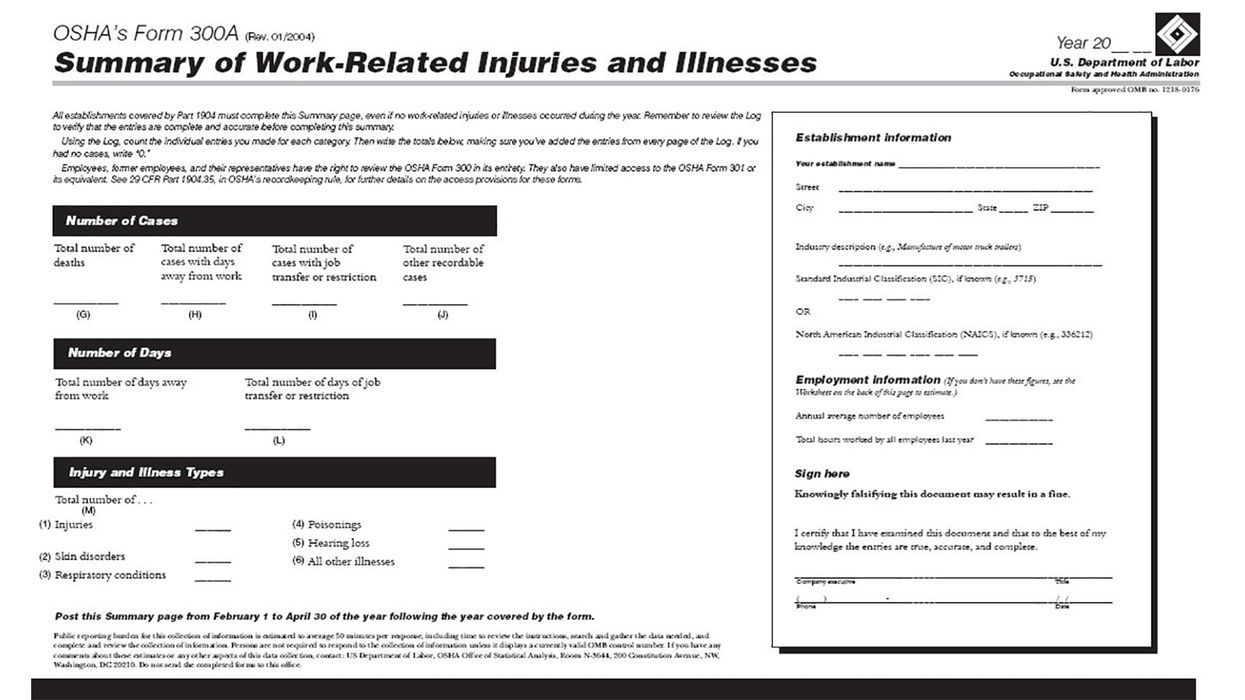
NewsIndustry NewsIndustry NewsEnforcement and Audits - OSHAOSHA InspectionsEnforcement and Audits - OSHASafety & HealthGeneral Industry SafetyOccupational Safety and Health Administration (OSHA), DOLEnglishFocus AreaUSA
2025-05-29T05:00:00Z
OSHA updates Site-Specific Targeting program
On May 20, OSHA updated its Site-Specific Targeting (SST) program to reflect the use of Form 300A data for calendar years (CY) 2021-2023. The SST program is OSHA’s primary planned inspection program for general industry establishments with 20 or more employees with the highest injury and illness rates.
Using Form 300A data from CY 2021-2023, OSHA may target establishments for inspection based on:
- High injury and illness rates from 2023 data.
- Upward trending injury and illness rates based on 2021-2023 data at or above twice the 2022 private sector average.
- Injury and illness rates markedly below industry averages.
- Failure to submit an OSHA Form 300A in 2023.
This update replaces the previous SST directive, issued in February 2023, which used CY 2019-2021 data.

NewsIndustry NewsSafety & HealthIn-Depth ArticleGeneral Industry SafetyHazardous Materials Safety - OSHAEnglishFocus AreaHazardous Materials Safety - OSHAUSA
2021-10-05T05:00:00Z
Safely handling battery acid spills
If employees charge forklift or other industrial batteries, they need to understand the hazards of acid and know how to handle small, incidental spills.
Battery acid is dilute sulfuric acid. Sulfuric acid is a clear, colorless liquid with an acrid smell. It’s corrosive and can cause severe burns.
In the event of a sulfuric acid/battery acid spill, employees should:
- Report the incident immediately.
- Neutralize the spill with soda ash or baking soda. Use one pound of baking soda to one gallon of water. Appropriate supplies should be near the charging area.
- The acid reaction is complete when it stops fizzing. Verify that the acid is neutralized by checking the pH with litmus paper or a pH meter. A neutral pH reading is between six and eight.
- Absorb neutralized material using material such as clay or kitty litter, if necessary. If the spill is very large, contain it with earth or clay dikes.
- Brush under battery connectors and remove all grime. Rinse the residue from the battery with clean water.
- Determine proper disposal by contacting local environmental authorities.
With proper training and supplies, employees can clean up battery acid spills safely.
NewsIndustry NewsSafety & HealthConstruction SafetyGeneral Industry SafetyFire Protection and PreventionIn-Depth ArticleEnglishFire Protection and PreventionFocus AreaUSA
2026-07-01T05:00:00Z
Fireworks outside, fire risks inside
July usually brings fireworks, cookouts, and a reminder that fire, when controlled, is part of the celebration. But in the workplace, fire is anything but a celebration. It’s one of those hazards that escalates fast, leaves little room for error, and demands that the basics are done right every single day.
It’s also more common than many realize. The National Fire Protection Association (NFPA) estimates U.S. fire departments respond to about 37,000 fires each year in industrial and manufacturing properties alone. For safety professionals, that’s the reality check. Fire prevention means putting the controls in place to stop fires from starting and preparing people to respond immediately if they do.
Start with the simple truth
Most workplace fires don’t come out of nowhere. They usually tie back to a few common issues:
- Housekeeping that slowly slips over time,
- Poor control or storage of combustible materials,
- Unmanaged ignition sources, and
- Equipment that isn’t maintained.
OSHA keeps it straightforward under 29 CFR 1910 Subpart E and Subpart L. Employers are expected to control fire hazards, maintain safe egress, and ensure fire protection systems are in place and working.
Housekeeping is still one of your best defenses
It sounds basic, but it’s one of the biggest gaps you’ll see on a shop floor or job site.
Dust, debris, waste materials, and even oily rags can turn into fuel if they’re not actively managed. OSHA 29 CFR 1910.22 requires workplaces to be kept clean and orderly, and 1910.106 addresses handling and storage of flammable liquids.
From a practical standpoint:
- Keep work areas clean and organized;
- Remove waste regularly, not “when we get to it”;
- Store flammables in approved containers and cabinets; and
- Check hidden areas like rafters, ducts, and equipment tops.
Control your ignition sources
Fire needs three things, fuel, oxygen, and an ignition source. You don’t always control oxygen, but you do control the other two.
Common ignition sources include:
- Damaged or overloaded electrical equipment;
- Hot work like welding, cutting, and grinding;
- Friction or heat from machinery; and
- Static discharge in certain environments.
OSHA and NFPA 51B (Standard for Fire Prevention During Welding, Cutting, and Other Hot Work) expectations are clear, you need controls, permits, and fire watches where applicable.
Make sure your protection systems actually protect
Having fire extinguishers, alarms, or sprinklers isn’t enough. They have to work when needed.
OSHA 1910.157 requires extinguishers to be properly selected for the hazards, kept accessible, inspected, and maintained so they’re ready to use. If someone grabs an extinguisher, it needs to work. Every time.
The same applies to alarms and suppression systems. OSHA 1910.165 requires fire alarms to provide a clear, reliable warning. Sprinkler systems under 1910.159 and fixed systems under 1910.160 must be inspected, tested, and maintained so they activate when needed.
Don’t overlook egress
When evacuating, people need a clear way out. Egress must be seamless, clear, direct, and easy to follow from wherever someone is working. If someone has to stop and figure it out, they’ve already lost time they don’t have.
OSHA 29 CFR 1910.36 and 1910.37 lay out the essentials including:
- Mark and light exit routes clearly,
- Keep exits and paths unobstructed,
- Avoid any storage or temporary blockages,
- Ensure doors open easily from the inside without keys or tools, and
- Make sure exits lead to a safe area.
Training has to be real, not just checked off
Fire events move fast, so there’s no time to figure it out on the fly. Training has to be simple, practical, and tied directly to the job. If workers can’t picture how it applies, it won’t stick when the unexpected happens.
At a minimum, training should cover:
- What causes fires in your workplace,
- How to prevent them,
- When to evacuate instead of fight a fire,
- When and how to use an extinguisher, and
- How to evacuate, including routes, meeting points, and accountability.
Just as important, employees need to be able to ask questions and understand what applies to their job. OSHA expects training to be effective, not just delivered.
Key takeaway: Fire safety comes down to consistent execution, clean work areas, maintained equipment, controlled hazards, and people who know what to do. Fires don’t give you a warning, so your controls have to be ready to work every time.
NewsEnforcement and Audits - OSHASafety and Health Programs and TrainingErgonomicsLockout/TagoutLockout/TagoutSafety and Health Programs and TrainingIn-Depth ArticleEnglishHeat StressErgonomicsOSHA Violations and PenaltiesIndustry NewsHeat and Cold ExposureSafety & HealthConstruction SafetyGeneral Industry SafetyAgriculture SafetyMaritime SafetyFocus AreaUSA
2026-06-24T05:00:00Z
Congress pushes OSHA and workplace safety in competing directions
A divided Capitol Hill is sending mixed signals on workplace safety policy. Some lawmakers are pressing for greater worker protection while others seek to block new rulemaking. Yet there is agreement that emerging safety challenges are on the rise. How these competing priorities will influence the OSHA landscape remains to be seen.
Pushback over Heat proposal
Dominating the pack of recent legislation affecting safety and health is the Heat Workforce Standards Act (S. 4427). The bill, introduced on April 29 by Senator Bill Cassidy, M.D. (R-LA) seeks to stop OSHA from finalizing, implementing, or enforcing a Heat Injury and Illness Prevention standard based on or similar to the August 30, 2024, proposal. This legislation underscores how OSHA rulemakings can face resistance around feasibility and cost.
The Senator calls the OSHA proposed rule burdensome, overly prescriptive, one-size-fits-all, and nearly impossible for employers to comply with. The lawmaker also argues that the rule would raise costs for small businesses. He adds that the proposal, if promulgated, would cause confusion.
It should be noted that a companion bill in the House (H.R. 6213) was introduced last November. In addition, two bills (H.R. 4443 and S. 2298) introduced last July would require OSHA to issue a standard to protect workers from heat-related injuries and illnesses.
Efforts to expand worker protection
To commemorate Workers’ Memorial Day on April 28, Senator Bernie Sanders (I-VT) introduced the Protecting America’s Workers Act (S. 4413). The legislation would reform the Occupational Safety and Health Act (OSH Act) to:
- Impose higher monetary penalties and criminal charges;
- Protect whistleblowers who report unsafe working conditions;
- Mandate that OSHA investigate all cases of workplace deaths or serious injuries;
- Require employers to inform workers of their right to a safe workplace; and
- Extend safety and health protections to federal, state, and local public employees.
This bill is a companion to last year’s House bill (H.R. 3036) by the same name. Both bills work to expand OSHA’s authority.
Emerging safety and health challenges
The House Workforce Protections Subcommittee held a hearing on May 14 to help shape the conversation about evolving workplace safety and health issues. Subcommittee Chairman Ryan Mackenzie (R-PA) explained that the idea was to “better prevent serious injuries and fatalities in the modern workplace.” Those who testified spoke about:
- Leading indicators,
- Safety and health management systems,
- Artificial intelligence,
- Advances in lockout/tagout systems,
- Worker wellbeing,
- Work violence,
- Opioid overdoses,
- Cannabis impairment,
- Silica dust exposure,
- New chemical exposures,
- Heat illness,
- Vehicle driving risks,
- Performance-based OSHA standards rather than prescriptive ones, and
- An accelerated OSHA variance program for new technologies.
Information from the hearing may shape future legislation or OSHA regulations.
Worker safety in meat plants
Senator Cory Booker (D-NJ) and four other legislators sent a letter to the U.S. Department of Agriculture (USDA) on April 30. The letter opposes the department’s proposed rules that would increase line speeds for poultry and swine processing plants. The lawmakers also oppose the removal of requirements for these establishments to submit annual worker safety data called attestations.
The letter urges USDA not to move forward with the proposals. It points to the USDA’s research on musculoskeletal disorders among poultry and swine slaughter workers. The letter also spotlights amputations in poultry facilities and meatpacking.
When USDA issued its research in 2025, Acting Labor Secretary Julie Su stated, “The findings in USDA's report on worker safety in poultry and swine plants show that injuries, including chronic pain and musculoskeletal disorders are too common. These kinds of injuries often go unreported. The study found that the increased risk of injuries created by increasing line speeds could be mitigated with other controls, specifically having more workers on the line and having effective ergonomic plans.”
While OSHA does not set line speeds in food plants, the issue illustrates how workplace safety is related to policy decisions in other agencies.
Consensus standards targeted
Another piece of legislation introduced March 19 seeks to provide public access to incorporated by reference consensus standards without requiring payment. Some standards are made freely available online, but not all.
The Pro Codes Act (S. 4145), if passed, would ensure that a consensus standard does not lose its copyright protection simply because it is incorporated by reference into law or regulation. However, the catch is the standard must be available for free viewing on a publicly accessible website. That website would be searchable. Plus, the standards organization could not use any personally identifiable information of site visitors without their consent.
Senator Chris Coons (D-DE) said of his bill, “This bipartisan legislation … will make the public safer by ensuring non-profits know they can develop better standards without fear of losing them.”
A companion House bill (H.R. 4072) by the same name was introduced in June last year.
Key to remember
In recent months, lawmakers have turned their attention to five areas impacting safety — blocking OSHA’s Heat proposal, strengthening the OSH Act, exploring emerging workplace safety issues, opposing faster line speeds, and increasing access to consensus standards.
NewsEmergency Planning - OSHAIndustry NewsSafety & HealthEmergency Planning (OSHA)General Industry SafetyExit RoutesEmergency ExitsIn-Depth ArticleEnglishFocus AreaUSA
2022-03-30T05:00:00Z
When an exit is not an exit
Depending on the size of your facility, you may have tens or hundreds, if not thousands, of doors. Knowing which doors to identify as an exit (or not an exit for that matter) can assist your employees in evacuation procedures. OSHA can sometimes use broad language, which can create an impression that nearly every door must be marked either “Not an exit” or marked for its actual use. It’s important to read further into the regulation and understand what OSHA actually requires.
Breaking down the regulation
Let’s start with the first part of the “Maintenance, safeguards, and operations features for exit route” regulation.
- 1910.37(b)(5): “each doorway or passage along an exit access that could be mistaken for an exit must be marked “Not an exit” or similar designation or be identified by a sign indicating its actual use (e.g., closet).”
- Per the definition in 1910.34, “Exit access means that portion of an exit route that leads to an exit. An example of an exit access is a corridor on the fifth floor of an office building that leads to a two-hour fire resistance-rated enclosed stairway (the Exit).”
We understand that wherever people are working, they probably follow a corridor or hallway, and those passages might potentially be part of an “exit access.” However, you might start your focus on the designated exit routes (as shown on evacuation maps) since those should be the primary doors of concern.
There’s more to read into this regulation.
- 1910.37(b)(5): “each doorway or passage along an exit access that could be mistaken for an exit must be marked “Not an exit” or similar designation or be identified by a sign indicating its actual use (e.g., closet).”
You’ll want to evaluate whether certain doors “could be mistaken” for an exit. Things like office doors are unlikely to be mistaken for an exit. Similarly, restrooms are usually marked as such, so they are “identified by a sign indicating actual use.” Potentially, areas like conference rooms are also marked (and potentially unlikely to be mistaken for an exit). Likewise, if you have increased your building footprint, and doors which used to lead outside now open into a new indoor area, you would want to mark those doors as “Not an exit” if they are as such.
Before you go out and spend your entire safety budget on “Exit” and “Not an exit” signage, remember that this regulation leaves open some subjectivity for interpretation.
Key to remember: Review your facility emergency action plan, look at your designated evacuation routes, and take a walk to see what signs currently exist. Not every door or passage will be along an exit access, and not every door or passage will have the potential to be mistaken for an exit.

NewsIndustry NewsAccident Investigation - OSHAAccident Investigation - OSHASafety & HealthConstruction SafetyGeneral Industry SafetyIn-Depth ArticleEnglishFocus AreaUSA
2026-06-16T05:00:00Z
Tank implosion tragedy highlights pressure hazards
A May 2026 incident at a paper mill in Washington put a spotlight on a hazard that doesn’t always get the same attention as over-pressure, vacuum induced tank collapse. The event involved a large chemical storage vessel and led to multiple fatalities and serious injuries. The U.S. Chemical Safety and Hazard Investigation Board (CSB) has opened an investigation to figure out what went wrong and how to keep it from happening again.
While that investigation plays out, there’s a clear takeaway, tank failures aren’t just an over-pressure problem. Vacuum conditions, or under pressure, can be just as destructive. We design for it, we talk about it, but it doesn’t always get the same focus in day‑to‑day operations, maintenance, or hazard reviews, and that’s where things can break down.
Understanding what happened
An implosion happens when the pressure inside a tank drops below the pressure outside it. When that happens, the outside air pushes in and the tank can collapse. Most people think about explosions. Fewer think about implosions. But the damage can be just as severe.
The tricky part is how this can develop during normal work. It doesn’t take a rare event and can happen during everyday tasks like:
- Draining a tank too fast without letting air flow back in;
- Cooling vapors or condensing material inside the tank;
- Steam cleaning and then cooling things down too quickly; and
- Vents that are blocked, closed, or just not sized right.
In industries like pulp and paper, chemical processing, and wastewater treatment, these situations aren’t unusual. In many cases, they’re part of day-to-day operations. That’s what makes vacuum-induced failure a real risk and a preventable one.
What OSHA expects for tank safety
While this incident puts a spotlight on an implosion hazard, OSHA’s expectations go beyond just one type of failure. The focus is on overall tank and pressure vessel safety, which includes both over-pressure and vacuum conditions.
Under the General Duty Clause, employers are required to protect workers from recognized hazards. Tank failure, whether it’s caused by pressure or vacuum, is a known risk, so OSHA expects it to be addressed. In practice, that means employers need to:
- Design for how the system actually operates, including pressure going in both directions;
- Control pressure risks with properly sized relief devices and venting systems that work when needed;
- Follow recognized engineering practices like ASME (American Society of Mechanical Engineers) and API (American Petroleum Institute) standards; and
- Keep equipment in good shape through inspection, testing, and maintenance.
Additionally, if Process Safety Management (29 CFR 1910.119) applies, expectations get more specific. Employers need to have:
- A mechanical integrity program that covers tanks and relief systems;
- Process hazard analyses that look at normal operations, abnormal conditions, and maintenance work; and
- Clear procedures and training so people know how to manage the risks.
Even if PSM doesn’t apply, the expectation doesn’t change. You still need to understand how the system can fail and make sure the right protections are in place.
Strengthening tank safety where it counts
This incident is a good reminder to take a step back and look at your organization’s overall tank and pressure vessel safety, not just one specific hazard. Strong programs come down to solid controls and making sure they hold up in day-to-day operations. Here’s where to focus your attention:
- Evaluate all pressure scenarios: Consider both over-pressure and vacuum conditions during normal, shutdown, and when things don’t go as planned;
- Verify relief and venting systems: Ensure devices are properly sized, installed, and not isolated or obstructed;
- Confirm design limits: Validate that tanks are rated for the full range of expected conditions;
- Strengthen inspection and maintenance: Regularly check vents, valves, and vessel integrity as part of a structured program; and
- Train employees on system behavior: Help operators understand how everyday actions, like emptying a tank, rinsing it out, or closing vents, can affect pressure conditions.
Key to remember: Expectation is clear, tanks must be safe under all operating conditions, not just ideal ones. That only happens when design, controls, and maintenance all line up with how the system really runs.
Saved to my EVENT CALENDAR!
View your saved links by clicking the arrow next to your profile picture located in the header. Then, click “My Activity” to view the Event Calendar on your Activity page.
OK
J. J. Keller is the trusted source for DOT / Transportation, OSHA / Workplace Safety, Human Resources, Construction Safety and Hazmat / Hazardous Materials regulation compliance products and services. J. J. Keller helps you increase safety awareness, reduce risk, follow best practices, improve safety training, and stay current with changing regulations.
Copyright 2026 J. J. Keller & Associate, Inc. For re-use options please contact copyright@jjkeller.com or call 800-558-5011.