Compliance Just Got Easier: Stay ahead of regulatory changes with instant notifications on updates that matter.
['Toxic and Hazardous Substances - OSHA']
['Toxic and Hazardous Substances - OSHA', 'Cadmium']
10/09/2023

Copyright 2026 J. J. Keller & Associate, Inc. For re-use options please contact copyright@jjkeller.com or call 800-558-5011.
1.00 Introduction
Under the final OSHA cadmium rule ( 29 CFR part 1910 ), monitoring of biological specimens and several periodic medical examinations are required for eligible employees. These medical examinations are to be conducted regularly, and medical monitoring is to include the periodic analysis of cadmium in blood (CDB), cadmium in urine (CDU) and beta-2-microglobulin in urine (B2MU). As CDU and B2MU are to be normalized to the concentration of creatinine in urine (CRTU), then CRTU must be analyzed in conjunction with CDU and B2MU analyses.
The purpose of this protocol is to provide procedures for establishing and maintaining the quality of the results obtained from the analyses of CDB, CDU and B2MU by commercial laboratories. Laboratories conforming to the provisions of this nonmandatory protocol shall be known as �participating laboratories.� The biological monitoring data from these laboratories will be evaluated by physicians responsible for biological monitoring to determine the conditions under which employees may continue to work in locations exhibiting airborne-cadmium concentrations at or above defined actions levels (see Paragraphs (l)(3) and (l)(4) of the final rule). These results also may be used to support a decision to remove workers from such locations.
Under the medical monitoring program for cadmium, blood and urine samples must be collected at defined intervals from workers by physicians responsible for medical monitoring; these samples are sent to commercial laboratories that perform the required analyses and report results of these analyses to the responsible physicians. To ensure the accuracy and reliability of these laboratory analyses, the laboratories to which samples are submitted should participate in an ongoing and efficacious proficiency testing program. Availability of proficiency testing programs may vary with the analyses performed.
To test proficiency in the analysis of CDB, CDU and B2MU, a laboratory should participate either in the interlaboratory comparison program operated by the Centre de Toxicologie du Quebec (CTQ) or an equivalent program. (Currently, no laboratory in the U.S. performs proficiency testing on CDB, CDU or B2MU.) Under this program, CTQ sends participating laboratories 18 samples of each analyte (CDB, CDU and/or B2MU) annually for analysis. Participating laboratories must return the results of these analyses to CTQ within four to five weeks after receiving the samples.
The CTQ program pools analytical results from many participating laboratories to derive consensus mean values for each of the samples distributed. Results reported by each laboratory then are compared against these consensus means for the analyzed samples to determine the relative performance of each laboratory. The proficiency of a participating laboratory is a function of the extent of agreement between results submitted by the participating laboratory and the consensus values for the set of samples analyzed.
Proficiency testing for CRTU analysis (which should be performed with CDU and B2MU analyses to evaluate the results properly) also is recommended. In the U.S., only the College of American Pathologists (CAP) currently conducts CRTU proficiency testing; participating laboratories should be accredited for CRTU analysis by the CAP.
Results of the proficiency evaluations will be forwarded to the participating laboratory by the proficiency-testing laboratory, as well as to physicians designated by the participating laboratory to receive this information. In addition, the participating laboratory should, on request, submit the results of their internal Quality Assurance/Quality Control (QA/QC) program for each analytic procedure (i.e., CDB, CDU and/or B2MU) to physicians designated to receive the proficiency results. For participating laboratories offering CDU and/or B2MU analyses, QA/QC documentation also should be provided for CRTU analysis. (Laboratories should provide QA/QC information regarding CRTU analysis directly to the requesting physician if they perform the analysis in-house; if CRTU analysis is performed by another laboratory under contract, this information should be provided to the physician by the contract laboratory.)
QA/QC information, along with the actual biological specimen measurements, should be provided to the responsible physician using standard formats. These physicians then may collate the QA/QC information with proficiency test results to compare the relative performance of laboratories, as well as to facilitate evaluation of the worker monitoring data. This information supports decisions made by the physician with regard to the biological monitoring program, and for mandating medical removal.
This protocol describes procedures that may be used by the responsible physicians to identify laboratories most likely to be proficient in the analysis of samples used in the biological monitoring of cadmium; also provided are procedures for record keeping and reporting by laboratories participating in proficiency testing programs, and recommendations to assist these physicians in interpreting analytical results determined by participating laboratories. As the collection and handling of samples affects the quality of the data, recommendations are made for these tasks. Specifications for analytical methods to be used in the medical monitoring program are included in this protocol as well.
In conclusion, this document is intended as a supplement to characterize and maintain the quality of medical monitoring data collected under the final cadmium rule promulgated by OSHA (29 CFR part 1910). OSHA has been granted authority under the Occupational Safety and Health Act of 1970 to protect workers from the effects of exposure to hazardous substances in the work place and to mandate adequate monitoring of workers to determine when adverse health effects may be occurring. This non-mandatory protocol is intended to provide guidelines and recommendations to improve the accuracy and reliability of the procedures used to analyze the biological samples collected as part of the medical monitoring program for cadmium.
2.0 Definitions
When the terms below appear in this protocol, use the following definitions.
Accuracy: A measure of the bias of a data set. Bias is a systematic error that is either inherent in a method or caused by some artifact or idiosyncrasy of the measurement system. Bias is characterized by a consistent deviation (positive or negative) in the results from an accepted reference value.
Arithmetic Mean: The sum of measurements in a set divided by the number of measurements in a set.
Blind Samples: A quality control procedure in which the concentration of analyte in the samples should be unknown to the analyst at the time that the analysis is performed.
Coefficient of Variation: The ratio of the standard deviation of a set of measurements to the mean (arithmetic or geometric) of the measurements.
Compliance Samples: Samples from exposed workers sent to a participating laboratory for analysis.
Control Charts: Graphic representations of the results for quality control samples being analyzed by a participating laboratory.
Control Limits: Statistical limits which define when an analytic procedure exceeds acceptable Parameters; control limits provide a method of assessing the accuracy of analysts, laboratories, and discrete analytic runs.
Control Samples: Quality control samples.
F/T: The measured amount of an analyte divided by the theoretical value (defined below) for that analyte in the sample analyzed; this ratio is a measure of the recovery for a quality control sample.
Geometric Mean: The natural antilog of the mean of a set of natural log-transformed data.
Geometric Standard Deviation: The antilog of the standard deviation of a set of natural log-transformed data.
Limit of Detection: Using a predefined level of confidence, this is the lowest measured value at which some of the measured material is likely to have come from the sample.
Mean: A central tendency of a set of data; in this protocol, this mean is defined as the arithmetic mean (see definition of arithmetic mean above) unless stated otherwise.
Performance: A measure of the overall quality of data reported by a laboratory.
Pools: Groups of quality-control samples to be established for each target value (defined below) of an analyte. For the protocol provided in attachment 3, for example, the theoretical value of the quality control samples of the pool must be within a range defined as plus or minus (�) 50% of the target value. Within each analyte pool, there must be quality control samples of at least 4 theoretical values.
Precision: The extent of agreement between repeated, independent measurements of the same quantity of an analyte.
Proficiency: The ability to satisfy a specified level of analyte performance. Proficiency Samples: Specimens, the values of which are unknown to anyone at a participating laboratory, and which are submitted by a participating laboratory for proficiency testing.
Quality or Data Quality: A measure of the confidence in the measurement value.
Quality Control (QC) Samples: Specimens, the value of which is unknown to the analyst, but is known to the appropriate QA/QC personnel of a participating laboratory; when used as part of a laboratory QA/QC program, the theoretical values of these samples should not be known to the analyst until the analyses are complete. QC samples are to be run in sets consisting of one QC sample from each pool (see definition of �pools� above).
Sensitivity: For the purposes of this protocol, the limit of detection.
Standard Deviation: A measure of the distribution or spread of a data set about the mean; the standard deviation is equal to the positive square root of the variance, and is expressed in the same units as the original measurements in the data set.
Standards: Samples with values known by the analyst and used to calibrate equipment and to check calibration throughout an analytic run. In a laboratory QA/QC program, the values of the standards must exceed the values obtained for compliance samples such that the lowest standard value is near the limit of detection and the highest standard is higher than the highest compliance sample or QC sample. Standards of at least three different values are to be used for calibration, and should be constructed from at least 2 different sources.
Target Value: Those values of CDB, CDU or B2MU which trigger some action as prescribed in the medical surveillance section of the regulatory text of the final cadmium rule. For CDB, the target values are 5, 10 and 15 ?g/l. For CDU, the target values are 3, 7, and 15 ?g/g CRTU. For ? 2 MU, the target values are 300, 750, and 1500 ?g/g CRTU. (Note that target values may vary as a function of time.)
Theoretical Value (or Theoretical Amount): The reported concentration of a quality-control sample (or calibration standard) derived from prior characterizations of the sample.
Value or Measurement Value: The numerical result of a measurement.
Variance: A measure of the distribution or spread of a data set about the mean; the variance is the sum of the squares of the differences between the mean and each discrete measurement divided by one less than the number of measurements in the data set.
3.0 Protocol
This protocol provides procedures for characterizing and maintaining the quality of analytic results derived for the medical monitoring program mandated for workers under the final cadmium rule.
3.1 Overview
The goal of this protocol is to assure that medical monitoring data are of sufficient quality to facilitate proper interpretation. The data quality objectives (DQOs) defined for the medical monitoring program are summarized in Table 1. Based on available information, the DQOs presented in Table 1 should be achievable by the majority of laboratories offering the required analyses commercially; OSHA recommends that only laboratories meeting these DQOs be used for the analysis of biological samples collected for monitoring cadmium exposure.
| Analyte/concentration pool | Limit of detection | Precision (CV) (%) | Accuracy |
|---|---|---|---|
| Cadmium in blood | 0.5 ?g/l | �1 ?g/l or 15% of the mean. | |
| ?2 ?g/l | 40 | ||
| >2 ?g/l | 20 | ||
| Cadmium in urine | 0.5 ?g/g creatinine | �1 ?g/l or 15% of the mean. | |
| ?2 ?g/l creatinine | 40 | ||
| >2 ?g/l creatinine | 20 | ||
| ?-2-microglobulin in urine: 100 ?g/g creatine. | 100 ?g/g creatinine | 5 | �15% of the mean. |
To satisfy the DQOs presented in Table 1, OSHA provides the following guidelines:
1. Procedures for the collection and handling of blood and urine are specified (Section 3.4.1 of this protocol);
2. Preferred analytic methods for the analysis of CDB, CDU and B2MU are defined (and a method for the determination of CRTU also is specified since CDU and B2MU results are to be normalized to the level of CRTU).
3. Procedures are described for identifying laboratories likely to provide the required analyses in an accurate and reliable manner;
4. These guidelines (Sections 3.2.1 to 3.2.3, and Section 3.3) include recommendations regarding internal QA/QC programs for participating laboratories, as well as levels of proficiency through participation in an interlaboratory proficiency program;
5. Procedures for QA/QC record keeping (Section 3.3.2), and for reporting QC/QA results are described (Section 3.3.3); and,
6. Procedures for interpreting medical monitoring results are specified (Section 3.4.3).
Methods recommended for the biological monitoring of eligible workers are:
1. The method of Stoeppler and Brandt (1980) for CDB determinations (limit of detection: 0.5 ?g/l);
2. The method of Pruszkowska et al. (1983) for CDU determinations (limit of detection: 0.5 ?g/l of urine); and,
3. The Pharmacia Delphia test kit (Pharmacia 1990) for the determination of B2MU (limit of detection: 100 ?g/l urine).
Because both CDU and B2MU should be reported in ?g/g CRTU, an independent determination of CRTU is recommended. Thus, both the OSHA Salt Lake City Technical Center (OSLTC) method (OSHA, no date) and the Jaffe method (Du Pont, no date) for the determination of CRTU are specified under this protocol (i.e., either of these 2 methods may be used). Note that although detection limits are not reported for either of these CRTU methods, the range of measurements expected for CRTU (0.9�1.7 ?g/l) are well above the likely limit of detection for either of these methods (Harrison, 1987).
Laboratories using alternate methods should submit sufficient data to the responsible physicians demonstrating that the alternate method is capable of satisfying the defined data quality objectives of the program. Such laboratories also should submit a QA/QC plan that documents the performance of the alternate method in a manner entirely equivalent to the QA/QC plans proposed in Section 3.3.1.
3.2 Duties of the Responsible Physician
The responsible physician will evaluate biological monitoring results provided by participating laboratories to determine whether such laboratories are proficient and have satisfied the QA/QC recommendations. In determining which laboratories to employ for this purpose, these physicians should review proficiency and QA/QC data submitted to them by the participating laboratories.
Participating laboratories should demonstrate proficiency for each analyte (CDU, CDB and B2MU) sampled under the biological monitoring program. Participating laboratories involved in analyzing CDU and B2MU also should demonstrate proficiency for CRTU analysis, or provide evidence of a contract with a laboratory proficient in CRTU analysis.
3.2.1 Recommendations for Selecting Among Existing Laboratories
OSHA recommends that existing laboratories providing commercial analyses for CDB, CDU and/or B2MU for the medical monitoring program satisfy the following criteria:
1. Should have performed commercial analyses for the appropriate analyte (CDB, CDU and/or B2MU) on a regular basis over the last 2 years;
2. Should provide the responsible physician with an internal QA/QC plan;
3. If performing CDU or B2MU analyses, the participating laboratory should be accredited by the CAP for CRTU analysis, and should be enrolled in the corresponding CAP survey (note that alternate credentials may be acceptable, but acceptability is to be determined by the responsible physician); and,
4. Should have enrolled in the CTQ interlaboratory comparison program for the appropriate analyte (CDB, CDU and/or B2MU).
Participating laboratories should submit appropriate documentation demonstrating compliance with the above criteria to the responsible physician. To demonstrate compliance with the first of the above criteria, participating laboratories should submit the following documentation for each analyte they plan to analyze (note that each document should cover a period of at least 8 consecutive quarters, and that the period designated by the term �regular analyses� is at least once a quarter):
1. Copies of laboratory reports providing results from regular analyses of the appropriate analyte (CDB, CDU and/or B2MU);
2. Copies of 1 or more signed and executed contracts for the provision of regular analyses of the appropriate analyte (CDB, CDU and/or B2MU); or,
3. Copies of invoices sent to 1 or more clients requesting payment for the provision of regular analyses of the appropriate analyte (CDB, CDU and/or B2MU). Whatever the form of documentation submitted, the specific analytic procedures conducted should be identified directly. The forms that are copied for submission to the responsible physician also should identify the laboratory which provided these analyses.
To demonstrate compliance with the second of the above criteria, a laboratory should submit to the responsible physician an internal QA/QC plan detailing the standard operating procedures to be adopted for satisfying the recommended QA/QC procedures for the analysis of each specific analyte (CDB, CDU and/or B2MU). Procedures for internal QA/QC programs are detailed in Section 3.3.1 below.
To satisfy the third of the above criteria, laboratories analyzing for CDU or B2MU also should submit a QA/QC plan for creatinine analysis (CRTU); the QA/QC plan and characterization analyses for CRTU must come from the laboratory performing the CRTU analysis, even if the CRTU analysis is being performed by a contract laboratory.
Laboratories enrolling in the CTQ program (to satisfy the last of the above criteria) must remit, with the enrollment application, an initial fee of approximately $100 per analyte. (Note that this fee is only an estimate, and is subject to revision without notice.) Laboratories should indicate on the application that they agree to have proficiency test results sent by the CTQ directly to the physicians designated by participating laboratories.
Once a laboratory�s application is processed by the CTQ, the laboratory will be assigned a code number which will be provided to the laboratory on the initial confirmation form, along with identification of the specific analytes for which the laboratory is participating. Confirmation of participation will be sent by the CTQ to physicians designated by the applicant laboratory.
3.2.2 Recommended Review of Laboratories Selected to Perform Analyses
Six months after being selected initially to perform analyte determinations, the status of participating laboratories should be reviewed by the responsible physicians. Such reviews should then be repeated every 6 months or whenever additional proficiency or QA/QC documentation is received (whichever occurs first).
As soon as the responsible physician has received the CTQ results from the first 3 rounds of proficiency testing (i.e., 3 sets of 3 samples each for CDB, CDU and/or B2MU) for a participating laboratory, the status of the laboratory�s continued participation should be reviewed. Over the same initial 6-month period, participating laboratories also should provide responsible physicians the results of their internal QA/QC monitoring program used to assess performance for each analyte (CDB, CDU and/or B2MU) for which the laboratory performs determinations. This information should be submitted using appropriate forms and documentation.
The status of each participating laboratory should be determined for each analyte (i.e., whether the laboratory satisfies minimum proficiency guidelines based on the proficiency samples sent by the CTQ and the results of the laboratory�s internal QA/QC program). To maintain competency for analysis of CDB, CDU and/or B2MU during the first review, the laboratory should satisfy performance requirements for at least 2 of the 3 proficiency samples provided in each of the 3 rounds completed over the 6-month period. Proficiency should be maintained for the analyte(s) for which the laboratory conducts determinations.
To continue participation for CDU and/or B2MU analyse, laboratories also should either maintain accreditation for CRTU analysis in the CAP program and participate in the CAP surveys, or they should contract the CDU and B2MU analyses to a laboratory which satisfies these requirements (or which can provide documentation of accreditation/participation in an equivalent program).
The performance requirement for CDB analysis is defined as an analytical result within � 1 ?g/l blood or 15% of the consensus mean (whichever is greater). For samples exhibiting a consensus mean less than 1 ?g/l, the performance requirement is defined as a concentration between the detection limit of the analysis and a maximum of 2 ?g/l. The purpose for redefining the acceptable interval for low CDB values is to encourage proper reporting of the actual values obtained during measurement; laboratories, therefore, will not be penalized (in terms of a narrow range of acceptability) for reporting measured concentrations smaller than 1 ?g/l.
The performance requirement for CDU analysis is defined as an analytical result within � 1 ?g/l urine or 15% of the consensus mean (whichever is greater). For samples exhibiting a consensus mean less than 1 ?g/l urine, the performance requirement is defined as a concentration between the detection limit of the analysis and a maximum of 2 ?g/l urine. Laboratories also should demonstrate proficiency in creatinine analysis as defined by the CAP. Note that reporting CDU results, other than for the CTQ proficiency samples should be accompanied with results of analyses for CRTU, and these 2 sets of results should be combined to provide a measure of CDU in units of ?g/g CRTU.
The performance requirement for B2MU is defined as analytical results within � 15% of the consensus mean. Note that reporting B2MU results, other than for CTQ proficiency samples should be accompanied with results of analyses for CRTU, and these 2 sets of results should be combined to provide a measure of B2MU in units of ?g/g CRTU.
There are no recommended performance checks for CRTU analyses. As stated previously, laboratories performing CRTU analysis in support of CDU or B2MU analyses should be accredited by the CAP, and participating in the CAP�s survey for CRTU.
Following the first review, the status of each participating laboratory should be reevaluated at regular intervals (i.e., corresponding to receipt of results from each succeeding round of proficiency testing and submission of reports from a participating laboratory�s internal QA/QC program).
After a year of collecting proficiency test results, the following proficiency criterion should be added to the set of criteria used to determine the participating laboratory�s status (for analyzing CDB, CDU and/or B2MU): A participating laboratory should not fail performance requirements for more than 4 samples from the 6 most recent consecutive rounds used to assess proficiency for CDB, CDU and/or B2MU separately (i.e., a total of 18 discrete proficiency samples for each analyte). Note that this requirement does not replace, but supplements, the recommendation that a laboratory should satisfy the performance criteria for at least 2 of the 3 samples tested for each round of the program.
3.2.3 Recommendations for Selecting Among Newly-Formed Laboratories (or Laboratories that Previously Failed to Meet the Protocol Guidelines)
OSHA recommends that laboratories that have not previously provided commercial analyses of CDB, CDU and/or B2MU (or have done so for a period less than 2 years), or which have provided these analyses for 2 or more years but have not conformed previously with these protocol guidelines, should satisfy the following provisions for each analyte for which determinations are to be made prior to being selected to analyze biological samples under the medical monitoring program:
1. Submit to the responsible physician an internal QA/QC plan detailing the standard operating procedures to be adopted for satisfying the QA/QC guidelines (guidelines for internal QA/QC programs are detailed in Section 3.3.1);
2. Submit to the responsible physician the results of the initial characterization analyses for each analyte for which determinations are to be made;
3. Submit to the responsible physician the results, for the initial 6-month period, of the internal QA/QC program for each analyte for which determinations are to be made (if no commercial analyses have been conducted previously, a minimum of 2 mock standardization trials for each analyte should be completed per month for a 6-month period);
4. Enroll in the CTQ program for the appropriate analyte for which determinations are to be made, and arrange to have the CTQ program submit the initial confirmation of participation and proficiency test results directly to the designated physicians. Note that the designated physician should receive results from 3 completed rounds from the CTQ program before approving a laboratory for participation in the biological monitoring program;
5. Laboratories seeking participation for CDU and/or B2MU analyses should submit to the responsible physician documentation of accreditation by the CAP for CRTU analyses performed in conjunction with CDU and/or B2MU determinations (if CRTU analyses are conducted by a contract laboratory, this laboratory should submit proof of CAP accreditation to the responsible physician); and,
6. Documentation should be submitted on an appropriate form.
To participate in CDB, CDU and/or B2MU analyses, the laboratory should satisfy the above criteria for a minimum of 2 of the 3 proficiency samples provided in each of the 3 rounds of the CTQ program over a 6-month period; this procedure should be completed for each appropriate analyte. Proficiency should be maintained for each analyte to continue participation. Note that laboratories seeking participation for CDU or B2MU also should address the performance requirements for CRTU, which involves providing evidence of accreditation by the CAP and participation in the CAP surveys (or an equivalent program).
The performance requirement for CDB analysis is defined as an analytical result within � 1 ?g/l or 15% of the consensus mean (whichever is greater). For samples exhibiting a consensus mean less than 1 ?g/l, the performance requirement is defined as a concentration between the detection limit of the analysis and a maximum of 2 ?g/l. The purpose of redefining the acceptable interval for low CDB values is to encourage proper reporting of the actual values obtained during measurement; laboratories, therefore, will not be penalized (in terms of a narrow range of acceptability) for reporting measured concentrations less than 1 ?g/l.
The performance requirement for CDU analysis is defined as an analytical result within � 1 ?g/l urine or 15% of the consensus mean (whichever is greater). For samples exhibiting a consensus mean less than 1 ?g/l urine, the performance requirement is defined as a concentration that falls between the detection limit of the analysis and a maximum of 2 ?g/l urine. Performance requirements for the companion CRTU analysis (defined by the CAP) also should be met. Note that reporting CDU results, other than for CTQ proficiency testing, should be accompanied with results of CRTU analyses, and these 2 sets of results should be combined to provide a measure of CDU in units of ?g/g CRTU.
The performance requirement for B2MU is defined as an analytical result within � 15% of the consensus mean. Note that reporting B2MU results, other than for CTQ proficiency testing should be accompanied with results of CRTU analysis, these 2 sets of results should be combined to provide a measure of B2MU in units of ?g/g CRTU.
Once a new laboratory has been approved by the responsible physician for conducting analyte determinations, the status of this approval should be reviewed periodically by the responsible physician as per the criteria presented under Section 3.2.2.
Laboratories which have failed previously to gain approval of the responsible physician for conducting determinations of 1 or more analytes due to lack of compliance with the criteria defined above for existing laboratories (Section 3.2.1), may obtain approval by satisfying the criteria for newly-formed laboratories defined under this section; for these laboratories, the second of the above criteria may be satisfied by submitting a new set of characterization analyses for each analyte for which determinations are to be made.
Reevaluation of these laboratories is discretionary on the part of the responsible physician. Reevaluation, which normally takes about 6 months, may be expedited if the laboratory can achieve 100% compliance with the proficiency test criteria using the 6 samples of each analyte submitted to the CTQ program during the first 2 rounds of proficiency testing.
For laboratories seeking reevaluation for CDU or B2MU analysis, the guidelines for CRTU analyses also should be satisfied, including accreditation for CRTU analysis by the CAP, and participation in the CAP survey program (or accreditation/participation in an equivalent program).
3.2.4 Future Modifications to the Protocol Guidelines
As participating laboratories gain experience with analyses for CDB, CDU and B2MU, it is anticipated that the performance achievable by the majority of laboratories should improve until it approaches that reported by the research groups which developed each method. OSHA, therefore, may choose to recommend stricter performance guidelines in the future as the overall performance of participating laboratories improves.
3.3 Guidelines for Record Keeping and Reporting
To comply with these guidelines, participating laboratories should satisfy the above-stated performance and proficiency recommendations, as well as the following internal QA/QC, record keeping, and reporting provisions.
If a participating laboratory fails to meet the provisions of these guidelines, it is recommended that the responsible physician disapprove further analyses of biological samples by that laboratory until it demonstrates compliance with these guidelines. On disapproval, biological samples should be sent to a laboratory that can demonstrate compliance with these guidelines, at least until the former laboratory is reevaluated by the responsible physician and found to be in compliance.
The following record keeping and reporting procedures should be practiced by participating laboratories.
3.3.1 Internal Quality Assurance/Quality Control Procedures
Laboratories participating in the cadmium monitoring program should develop and maintain an internal quality assurance/quality control (QA/QC) program that incorporates procedures for establishing and maintaining control for each of the analytic procedures (determinations of CDB, CDU and/or B2MU) for which the laboratory is seeking participation. For laboratories analyzing CDU and/or B2MU, a QA/QC program for CRTU also should be established.
Written documentation of QA/QC procedures should be described in a formal QA/QC plan; this plan should contain the following information: sample acceptance and handling procedures (i.e., chain-of-custody); sample preparation procedures; instrument Parameters; calibration procedures; and, calculations. Documentation of QA/QC procedures should be sufficient to identify analytical problems, define criteria under which analysis of compliance samples will be suspended, and describe procedures for corrective actions.
3.3.1.1 QA/QC procedures for establishing control of CDB and CDU analyses
The QA/QC program for CDB and CDU should address, at a minimum, procedures involved in calibration, establishment of control limits, internal QC analyses and maintaining control, and corrective-action protocols. The participating laboratory should develop and maintain procedures to assure that analyses of compliance samples are within control limits, and that these procedures are documented thoroughly in a QA/QC plan.
A nonmandatory QA/QC protocol is presented in Attachment 1. This attachment is illustrative of the procedures that should be addressed in a proper QA/QC program.
Calibration. Before any analytic runs are conducted, the analytic instrument should be calibrated. Calibration should be performed at the beginning of each day on which QC and/or compliance samples are run. Once calibration is established, QC or compliance samples may be run. Regardless of the type of samples run, about every fifth sample should serve as a standard to assure that calibration is being maintained.
Calibration is being maintained if the standard is within �15% of its theoretical value. If a standard is more than � 15% of its theoretical value, the run has exceeded control limits due to calibration error; the entire set of samples then should be reanalyzed after recalibrating or the results should be recalculated based on a statistical curve derived from that set of standards.
It is essential that the value of the highest standard analyzed be higher than the highest sample analyzed; it may be necessary, therefore, to run a high standard at the end of the run, which has been selected based on results obtained over the course of the run (i.e., higher than any standard analyzed to that point).
Standards should be kept fresh; as samples age, they should be compared with new standards and replaced if necessary.
Internal Quality Control Analyses. Internal QC samples should be determined interspersed with analyses of compliance samples. At a minimum, these samples should be run at a rate of 5% of the compliance samples or at least one set of QC samples per analysis of compliance samples, whichever is greater. If only 2 samples are run, they should contain different levels of cadmium.
Internal QC samples may be obtained as commercially-available reference materials and/or they may be internally prepared. Internally-prepared samples should be well characterized and traced, or compared to a reference material for which a consensus value is available.
Levels of cadmium contained in QC samples should not be known to the analyst prior to reporting the results of the analysis.
Internal QC results should be plotted or charted in a manner which describes sample recovery and laboratory control limits.
Internal Control Limits. The laboratory protocol for evaluating internal QC analyses per control limits should be clearly defined. Limits may be based on statistical methods (e.g., as 2? from the laboratory mean recovery), or on proficiency testing limits (e.g., � 1 ?g or 15% of the mean, whichever is greater). Statistical limits that exceed � 40% should be reevaluated to determine the source error in the analysis.
When laboratory limits are exceeded, analytic work should terminate until the source of error is determined and corrected; compliance samples affected by the error should be reanalyzed. In addition, the laboratory protocol should address any unusual trends that develop which may be biasing the results. Numerous, consecutive results above or below laboratory mean recoveries, or outside laboratory statistical limits, indicate that problems may have developed.
Corrective Actions. The QA/QC plan should document in detail specific actions taken if control limits are exceeded or unusual trends develop. Corrective actions should be noted on an appropriate form, accompanied by supporting documentation.
In addition to these actions, laboratories should include whatever additional actions are necessary to assure that accurate data are reported to the responsible physicians.
Reference Materials. The following reference materials may be available:
Cadmium in Blood (CDB)
1. Centre de Toxicologie du Quebec, Le Centre Hospitalier de l�Universite Laval, 2705 boul. Laurier, Quebec, Que., Canada G1V 4G2. (Prepared 6 times per year at 1-15 ?g Cd/l.)
2. H. Marchandise, Community Bureau of Reference-BCR, Directorate General XII, Commission of the European Communities, 200, rue de la Loi, B-1049, Brussels, Belgium. (Prepared as Bl CBM-1 at 5.37 ?g Cd/l, and Bl CBM-2 at 12.38 ?g Cd/l.)
3. Kaulson Laboratories Inc., 691 Bloomfield Ave., Caldwell, NJ 07006; tel: (201) 226-9494, FAX (201) 226-3244. (Prepared as 0141 [As, Cd, Hg, Pb] at 2 levels.)
Cadmium in Urine (CDU)
1. Centre de Toxicologie du Quebec, Le Centre Hospitalier de l�Universite Laval, 2705 boul. Laurier, Quebec, Que., Canada G1V 4G2. (Prepared 6 times per year.)
2. National Institute of Standards and Technology (NIST), Dept. of Commerce, Gaithersburg, MD; tel: (301) 975-6776. (Prepared as SRM 2670 freeze-dried urine [metals]; set includes normal and elevated levels of metals; cadmium is certified for elevated level of 88.0 ?g/l in reconstituted urine.)
3. Kaulson Laboratories Inc., 691 Bloomfield Ave., Caldwell, NJ 07006; tel: (201) 226-9494, FAX (201) 226-3244. (Prepared as 0140 [As, Cd, Hg, Pb] at 2 levels.)
3.3.1.2 QA/QC procedures for establishing control of B2MU
A written, detailed QA/QC plan for B2MU analysis should be developed. The QA/QC plan should contain a protocol similar to those protocols developed for the CDB/CDU analyses. Differences in analyses may warrant some differences in the QA/QC protocol, but procedures to ensure analytical integrity should be developed and followed.
Examples of performance summaries that can be provided include measurements of accuracy (i.e., the means of measured values versus target values for the control samples) and precision (i.e., based on duplicate analyses). It is recommended that the accuracy and precision measurements be compared to those reported as achievable by the Pharma-cia Delphia kit (Pharmacia 1990) to determine if and when unsatisfactory analyses have arisen. If the measurement error of 1 or more of the control samples is more than 15%, the run exceeds control limits. Similarly, this decision is warranted when the average CV for duplicate samples is greater than 5%.
3.3.2 Procedures for Record Keeping
To satisfy reporting requirements for commercial analyses of CDB, CDU and/or B2MU performed for the medical monitoring program mandated under the cadmium rule, participating laboratories should maintain the following documentation for each analyte:
1. For each analytic instrument on which analyte determinations are made, records relating to the most recent calibration and QC sample analyses;
2. For these instruments, a tabulated record for each analyte of those determinations found to be within and outside of control limits over the past 2 years;
3. Results for the previous 2 years of the QC sample analyses conducted under the internal QA/QC program (this information should be: Provided for each analyte for which determinations are made and for each analytic instrument used for this purpose, sufficient to demonstrate that internal QA/QC programs are being executed properly, and consistent with data sent to responsible physicians.
4. Duplicate copies of monitoring results for each analyte sent to clients during the previous 5 years, as well as associated information; supporting material such as chain-of-custody forms also should be retained; and,
5. Proficiency test results and related materials received while participating in the CTQ interlaboratory program over the past 2 years; results also should be tabulated to provide a serial record of relative error (derived per Section 3.3.3 below).
3.3.3 Reporting Procedures
Participating laboratories should maintain these documents: QA/QC program plans; QA/QC status reports; CTQ proficiency program reports; and, analytical data reports. The information that should be included in these reports is summarized in Table 2; a copy of each report should be sent to the responsible physician.
| Report | Frequency (time frame) | Contents |
|---|---|---|
| 1 QA/QC Program Plan | Once (initially) | A detailed description of the QA/QC protocol to be established by the laboratory to maintain control of analyte determinations. |
| 2 QA/QC Status Report | Every 2 months | Results of the QC samples incorporated into regular runs for each instrument (over the period since the last report). |
| 3 Proficiency Report | Attached to every data report | Results from the last full year of proficiency samples submitted to the CTQ program and results of the 100 most recent QC samples incorporated into regular runs for each instrument. |
| 4 Analytical Data Report | For all reports of data results | Date the sample was received; Date the sample was analyzed; Appropriate chain-of-custody information; Types of analyses performed; Results of the requested analyses; and Copy of the most current proficiency report. |
As noted in Section 3.3.1, a QA/QC program plan should be developed that documents internal QA/QC procedures (defined under Section 3.3.1) to be implemented by the participating laboratory for each analyte; this plan should provide a list identifying each instrument used in making analyte determinations.
A QA/QC status report should be written bimonthly for each analyte. In this report, the results of the QC program during the reporting period should be reported for each analyte in the following manner: The number (N) of QC samples analyzed during the period; a table of the target levels defined for each sample and the corresponding measured values; the mean of F/T value (as defined below) for the set of QC samples run during the period; and, use of X � 2 � (as defined below) for the set of QC samples run during the period as a measure of precision.
As noted in Section 2, an F/T value for a QC sample is the ratio of the measured concentration of analyte to the established (i.e., reference) concentration of analyte for that QC sample. The equation below describes the derivation of the mean for F/T values, X, (with N being the total number of samples analyzed):
 |
The standard deviation, �, for these measurements is derived using the following equation (note that 2 � is twice this value):
 |
The nonmandatory QA/QC protocol (see Attachment 1) indicates that QC samples should be divided into several discrete pool, and a separate estimate of precision for each pool then should be derived. Several precision estimates should be provided for concentrations which differ in average value. These precision measures may be used to document improvements in performance with regard to the combined pool.
Participating laboratories should use the CTQ proficiency program for each analyte. Results of this program will be sent by CTQ directly to physicians designated by the participating laboratories. Proficiency results from the CTQ program are used to establish the accuracy of results from each participating laboratory, and should be provided to responsible physicians for use in trend analysis. A proficiency report consisting of these proficiency results should accompany data reports as an attachment.
For each analyte, the proficiency report should include the results from the 6 previous proficiency rounds in the following format:
1. Number (N) of samples analyzed;
2. Mean of the target levels, (1/N)?T i with T i being a consensus mean for the sample;
3. Mean of the measurements, (1/N)?M i with M i being a sample measurement;
4. A measure of error defined by: (1/N)?(T i � M i ) 2
Analytical data reports should be submitted to responsible physicians directly. For each sample, report the following information: The date the sample was received; the date the sample was analyzed; appropriate chain-of-custody information; the type(s) of analyses performed; and, the results of the analyses. This information should be reported on a form similar to the form provided an appropriate form. The most recent proficiency program report should accompany the analytical data reports (as an attachment).
Confidence intervals for the analytical results should be reported as X � 2 �, with X being the measured value and 2 � the standard deviation calculated as described above.
For CDU or B2MU results, which are combined with CRTU measurements for proper reporting, the 95% confidence limits are derived from the limits for CDU or B2MU, (p), and the limits for CRTU, (q), as follows:
 |
For these calculations, X � p is the measurement and confidence limits for CDU or B2MU, and Y � q is the measurement and confidence limit for CRTU.
Participating laboratories should notify responsible physicians as soon as they receive information indicating a change in their accreditation status with the CTQ or the CAP. These physicians should not be expected to wait until formal notice of a status change has been received from the CTQ or the CAP.
3.4 Instructions to Physicians
Physicians responsible for the medical monitoring of cadmium-exposed workers must collect the biological samples from workers; they then should select laboratories to perform the required analyses, and should interpret the analytic results.
3.4.1 Sample Collection and Holding Procedures
Blood Samples. The following procedures are recommended for the collection, shipment and storage of blood samples for CDB analysis to reduce analytical variability; these recommendations were obtained primarily through personal communications with J.P. Weber of the CTQ (1991), and from reports by the Centers for Disease Control (CDC, 1986) and Stoeppler and Brandt (1980).
To the extent possible, blood samples should be collected from workers at the same time of day. Workers should shower or thoroughly wash their hands and arms before blood samples are drawn. The following materials are needed for blood sample collection: Alcohol wipes; sterile gauze sponges; band-aids; 20-gauge, 1.5-in. stainless steel needles (sterile); preprinted labels; tourniquets; vacutainer holders; 3-ml �metal free� vacutainer tubes (i.e., dark-blue caps), with EDTA as an anti-coagulant; and, styrofoam vacutainer shipping containers.
Whole blood samples are taken by venipuncture. Each blue-capped tube should be labeled or coded for the worker and company before the sample is drawn. (Blue-capped tubes are recommended instead of redcapped tubes because the latter may consist of red coloring pigment containing cadmium, which could contaminate the samples.) Immediately after sampling, the vacutainer tubes must be thoroughly mixed by inverting the tubes at least 10 times manually or mechanically using a Vortex device (for 15 sec). Samples should be refrigerated immediately or stored on ice until they can be packed for shipment to the participating laboratory for analysis.
The CDC recommends that blood samples be shipped with a �cool pak� to keep the samples cold during shipment. However, the CTQ routinely ships and receives blood samples for cadmium analysis that have not been kept cool during shipment. The CTQ has found no deterioration of cadmium in biological fluids that were shipped via parcel post without a cooling agent, even though these deliveries often take 2 weeks to reach their destination.
Urine Samples. The following are recommended procedures for the collection, shipment and storage of urine for CDU and B2MU analyses, and were obtained primarily through personal communications with J.P. Weber of the CTQ (1991), and from reports by the CDC (1986) and Stoeppler and Brandt (1980).
Single �spot� samples are recommended. As B2M can degrade in the bladder, workers should first empty their bladder and then drink a large glass of water at the start of the visit. Urine samples then should be collected within 1 hour. Separate samples should be collected for CDU and B2MU using the following materials: Sterile urine collection cups (250 ml); small sealable plastic bags; preprinted labels; 15-ml polypropylene or polyethylene screw-cap tubes; lab gloves (�metal free�); and, preservatives (as indicated).
The sealed collection cup should be kept in the plastic bag until collection time. The workers should wash their hands with soap and water before receiving the collection cup. The collection cup should not be opened until just before voiding and the cup should be sealed immediately after filling. It is important that the inside of the container and cap are not touched by, or come into contact with, the body, clothing or other surfaces.
For CDU analyses, the cup is swirled gently to resuspend any solids, and the 15-ml tube is filled with 10-12 ml urine. The CDC recommends the addition of 100 ?l concentrated HNO 3 as a preservative before sealing the tube and then freezing the sample. The CTQ recommends minimal handling and does not acidify their interlaboratory urine reference materials prior to shipment, nor do they freeze the sample for shipment. At the CTQ, if the urine sample has much sediment, the sample is acidified in the lab to free any cadmium in the precipitate.
For B2M, the urine sample should be collected directly into a polyethylene bottle previously washed with dilute nitric acid. The pH of the urine should be measured and adjusted to 8.0 with 0.1 N NaOH immediately following collection. Samples should be frozen and stored at -20�C until testing is performed. The B2M in the samples should be stable for 2 days when stored at 2-8�C, and for at least 2 months at -20�C. Repeated freezing and thawing should be avoided to prevent denaturing the B2M (Pharmacia 1990).
3.4.2 Recommendations for Evaluating Laboratories
Using standard error data and the results of proficiency testing obtained from CTQ, responsible physicians can make an informed choice of which laboratory to select to analyze biological samples. In general, laboratories with small standard errors and little disparity between target and measured values tend to make precise and accurate sample determinations. Estimates of precision provided to the physicians with each set of monitoring results can be compared to previously-reported proficiency and precision estimates. The latest precision estimates should be at least as small as the standard error reported previously by the laboratory. Moreover, there should be no indication that precision is deteriorating (i.e., increasing values for the precision estimates). If precision is deteriorating, physicians may decide to use another laboratory for these analyses. QA/QC information provided by the participating laboratories to physicians can, therefore, assist physicians in evaluating laboratory performance.
3.4.3 Use and Interpretation of Results
When the responsible physician has received the CDB, CDU and/or B2MU results, these results must be compared to the action levels discussed in the final rule for cadmium. The comparison of the sample results to action levels is straightforward. The measured value reported from the laboratory can be compared directly to the action levels; if the reported value exceeds an action level, the required actions must be initiated.
4.0 Background
Cadmium is a naturally-occurring environmental contaminant to which humans are continually exposed in food, water, and air. The average daily intake of cadmium by the U.S. population is estimated to be 10-20 ?g/day. Most of this intake is via ingestion, for which absorption is estimated at 4-7% (Kowal et al. 1979). An additional nonoccupational source of cadmium is smoking tobacco; smoking a pack of cigarettes a day adds an additional 2-4 ?g cadmium to the daily intake, assuming absorption via inhalation of 25-35% (Nordberg and Nordberg 1988; Friberg and Elinder 1988; Travis and Haddock 1980).
Exposure to cadmium fumes and dusts in an occupational setting where air concentrations are 20-50 ?g/m 3 results in an additional daily intake of several hundred micrograms (Friberg and Elinder 1988, p. 563). In such a setting, occupational exposure to cadmium occurs primarily via inhalation, although additional exposure may occur through the ingestion of material via contaminated hands if workers eat or smoke without first washing. Some of the particles that are inhaled initially may be ingested when the material is deposited in the upper respiratory tract, where it may be cleared by mucociliary transport and subsequently swallowed.
Cadmium introduced into the body through inhalation or ingestion is transported by the albumin fraction of the blood plasma to the liver, where it accumulates and is stored principally as a bound form complexed with the protein metallothionein. Metallothionein-bound cadmium is the main form of cadmium subsequently transported to the kidney; it is these 2 organs, the liver and kidney, in which the majority of the cadmium body burden accumulates. As much as one half of the total body burden of cadmium may be found in the kidneys (Nordberg and Nordberg 1988).
Once cadmium has entered the body, elimination is slow; about 0.02% of the body burden is excreted per day via urinary/fecal elimination. The whole-body half-life of cadmium is 10-35 years, decreasing slightly with increasing age (Travis and Haddock 1980).
The continual accumulation of cadmium is the basis for its chronic noncarcinogenic toxicity. This accumulation makes the kidney the target organ in which cadmium toxicity usually is first observed (Piscator 1964). Renal damage may occur when cadmium levels in the kidney cortex approach 200 ?g/g wet tissue-weight (Travis and Haddock 1980).
The kinetics and internal distribution of cadmium in the body are complex, and depend on whether occupational exposure to cadmium is ongoing or has terminated. In general, cadmium in blood is related principally to recent cadmium exposure, while cadmium in urine reflects cumulative exposure (i.e., total body burden) (Lauwerys et al. 1976; Friberg and Elinder 1988).
4.1 Health Effects
Studies of workers in a variety of industries indicate that chronic exposure to cadmium may be linked to several adverse health effects including kidney dysfunction, reduced pulmonary function, chronic lung disease and cancer (Federal Register 1990). The primary sites for cadmium-associated cancer appear to be the lung and the prostate.
Cancer. Evidence for an association between cancer and cadmium exposure comes from both epidemiological studies and animal experiments. Pott (1965) found a statistically significant elevation in the incidence of prostate cancer among a cohort of cadmium workers. Other epidemiology studies also report an elevated incidence of prostate cancer; however, the increases observed in these other studies were not statistically significant (Meridian Research, Inc. 1989).
One study (Thun et al. 1985) contains sufficiently quantitative estimates of cadmium exposure to allow evaluation of dose-response relationships between cadmium exposure and lung cancer. A statistically significant excess of lung cancer attributed to cadmium exposure was found in this study, even after accounting for confounding variables such as coexposure to arsenic and smoking habits (Meridian Research, Inc. 1989).
Evidence for quantifying a link between lung cancer and cadmium exposure comes from a single study (Takenaka et al. 1983). In this study, dose-response relationships developed from animal data were extrapolated to humans using a variety of models. OSHA chose the multistage risk model for estimating the risk of cancer for humans using these animal data. Animal injection studies also suggest an association between cadmium exposure and cancer, particularly observations of an increased incidence of tumors at sites remote from the point of injection. The International Agency for Research on Cancer (IARC) (Supplement 7, 1987) indicates that this, and related, evidence is sufficient to classify cadmium as an animal carcinogen. However, the results of these injection studies cannot be used to quantify risks attendant to human occupational exposures due to differences in routes of exposure (Meridian Research, Inc. 1989).
Based on the above-cited studies, the U.S. Environmental Protection Agency (EPA) classifies cadmium as �B1,� a probable human carcinogen (USEPA 1985). IARC in 1987 recommended that cadmium be listed as a probable human carcinogen.
Kidney Dysfunction. The most prevalent nonmalignant effect observed among workers chronically exposed to cadmium is kidney dysfunction. Initially, such dysfunction is manifested by proteinuria (Meridian Research, Inc. 1989; Roth Associates, Inc. 1989). Proteinuria associated with cadmium exposure is most commonly characterized by excretion of low-molecular weight proteins (15,000-40,000 MW), accompanied by loss of electrolytes, uric acid, calcium, amino acids, and phosphate. Proteins commonly excreted include ?-2-microglobulin (B2M), retinol-binding protein (RBP), immunoglobulin light chains, and lysozyme. Excretion of low molecular weight proteins is characteristic of damage to the proximal tubules of the kidney (Iwao et al. 1980).
Exposure to cadmium also may lead to urinary excretion of high-molecular weight proteins such as albumin, immunoglobulin G, and glycoproteins (Meridian Research, Inc. 1989; Roth Associates, Inc. 1989). Excretion of high-molecular weight proteins is indicative of damage to the glomeruli of the kidney. Bernard et al. (1979) suggest that cadmium-associated damage to the glomeruli and damage to the proximal tubules of the kidney develop independently of each other, but may occur in the same individual.
Several studies indicate that the onset of low-molecular weight proteinuria is a sign of irreversible kidney damage (Friberg et al. 1974; Roels et al. 1982; Piscator 1984; Elinder et al. 1985; Smith et al. 1986). For many workers, once sufficiently elevated levels of B2M are observed in association with cadmium exposure, such levels do not appear to return to normal even when cadmium exposure is eliminated by removal of the worker from the cadmium-contaminated work environment (Friberg, exhibit 29, 1990).
Some studies indicate that cadmium-induced proteinuria may be progressive; levels of B2MU increase even after cadmium exposure has ceased (Elinder et al. 1985). Other researchers have reached similar conclusions (Frieburg testimony, OSHA docket exhibit 29, Elinder testimony, OSHA docket exhibit 55, and OSHA docket exhibits 8-86B). Such observations are not universal, however (Smith et al. 1986; Tsuchiya 1976). Studies in which proteinuria has not been observed, however, may have initiated the reassessment too early (Meridian Research, Inc.1989; Roth Associates, Inc. 1989; Roels 1989).
A quantitative assessment of the risks of developing kidney dysfunction as a result of cadmium exposure was performed using the data from Ellis et al. (1984) and Falck et al. (1983). Meridian Research, Inc. (1989) and Roth Associates, Inc. (1989) employed several mathematical models to evaluate the data from the 2 studies, and the results indicate that cumulative cadmium exposure levels between 5 and 100 ?g-years/m 3 correspond with a one-in-a-thousand probability of developing kidney dysfunction.
When cadmium exposure continues past the onset of early kidney damage (manifested as proteinuria), chronic nephrotoxicity may occur (Meridian Research, Inc. 1989; Roth Associates, Inc. 1989). Uremia, which is the loss of the glomerulus� ability to adequately filter blood, may result. This condition leads to severe disturbance of electrolyte concentrations, which may result in various clinical complications including atherosclerosis, hypertension, pericarditis, anemia, hemorrhagic tendencies, deficient cellular immunity, bone changes, and other problems. Progression of the disease may require dialysis or a kidney transplant.
Studies in which animals are chronically exposed to cadmium confirm the renal effects observed in humans (Friberg et al. 1986). Animal studies also confirm cadmium-related problems with calcium metabolism and associated skeletal effects, which also have been observed among humans. Other effects commonly reported in chronic animal studies include anemia, changes in liver morphology, immunosuppression and hypertension. Some of these effects may be associated with cofactors; hypertension, for example, appears to be associated with diet, as well as with cadmium exposure. Animals injected with cadmium also have shown testicular necrosis.
4.2 Objectives for Medical Monitoring
In keeping with the observation that renal disease tends to be the earliest clinical manifestation of cadmium toxicity, the final cadmium standard mandates that eligible workers must be medically monitored to prevent this condition (as well as cadmium-induced cancer). The objectives of medical monitoring, therefore, are to: Identify workers at significant risk of adverse health effects from excess, chronic exposure to cadmium; prevent future cases of cadmium-induced disease; detect and minimize existing cadmium-induced disease; and, identify workers most in need of medical intervention.
The overall goal of the medical monitoring program is to protect workers who may be exposed continuously to cadmium over a 45-year occupational lifespan. Consistent with this goal, the medical monitoring program should assure that:
1. Current exposure levels remain sufficiently low to prevent the accumulation of cadmium body burdens sufficient to cause disease in the future by monitoring CDB as an indicator of recent cadmium exposure;
2. Cumulative body burdens, especially among workers with undefined historical exposures, remain below levels potentially capable of leading to damage and disease by assessing CDU as an indicator of cumulative exposure to cadmium; and,
3. Health effects are not occurring among exposed workers by determining B2MU as an early indicator of the onset of cadmium-induced kidney disease.
4.3 Indicators of Cadmium Exposure and Disease
Cadmium is present in whole blood bound to albumin, in erythrocytes, and as a metallothionein-cadmium complex. The metallothionein-cadmium complex that represents the primary transport mechanism for cadmium delivery to the kidney. CDB concentrations in the general, nonexposed population average 1 ?g Cd/l whole blood, with smokers exhibiting higher levels (see Section 5.1.6). Data presented in Section 5.1.6 shows that 95% of the general population not occupationally exposed to cadmium have CDB levels less than 5 ?g Cd/l.
If total body burdens of cadmium remain low, CDB concentrations indicate recent exposure (i.e., daily intake). This conclusion is based on data showing that cigarette smokers exhibit CDB concentrations of 2-7 ?g/l depending on the number of cigarettes smoked per day (Nordberg and Nordberg 1988), while CDB levels for those who quit smoking return to general population values (approximately 1 ?g/l) within several weeks (Lauwerys et al. 1976). Based on these observations, Lauwerys et al. (1976) concluded that CDB has a biological half-life of a few weeks to less than 3 months. As indicated in Section 3.1.6, the upper 95th percentile for CDB levels observed among those who are not occupationally exposed to cadmium is 5 ?g/l, which suggests that the absolute upper limit to the range reported for smokers by Nordberg and Nordberg may have been affected by an extreme value (i.e., beyond 2? above the mean).
Among occupationally-exposed workers, the occupational history of exposure to cadmium must be evaluated to interpret CDB levels. New workers, or workers with low exposures to cadmium, exhibit CDB levels that are representative of recent exposures, similar to the general population. However, for workers with a history of chronic exposure to cadmium, who have accumulated significant stores of cadmium in the kidneys/liver, part of the CDB concentrations appear to indicate body burden. If such workers are removed from cadmium exposure, their CDB levels remain elevated, possibly for years, reflecting prior long-term accumulation of cadmium in body tissues. This condition tends to occur, however, only beyond some threshold exposure value, and possibly indicates the capacity of body tissues to accumulate cadmium which cannot be excreted readily (Friberg and Elinder 1988; Nordberg and Nordberg 1988).
CDU is widely used as an indicator of cadmium body burdens (Nordberg and Nordberg 1988). CDU is the major route of elimination and, when CDU is measured, it is commonly expressed either as ?g Cd/l urine (unadjusted), ?g Cd/l urine (adjusted for specific gravity), or ?g Cd/g CRTU (see Section 5.2.1). The metabolic model for CDU is less complicated than CDB, since CDU is dependent in large part on the body (i.e., kidney) burden of cadmium. However, a small proportion of CDU still may be attributed to recent cadmium exposure, particularly if exposure to high airborne concentrations of cadmium occurred. Note that CDU is subject to larger interindividual and day-to-day variations than CDB, so repeated measurements are recommended for CDU evaluations.
CDU is bound principally to metallothionein, regardless of whether the cadmium originates from metallothionein in plasma or from the cadmium pool accumulated in the renal tubules. Therefore, measurement of metallothionein in urine may provide information similar to CDU, while avoiding the contamination problems that may occur during collection and handling urine for cadmium analysis (Nordberg and Nordberg 1988). However, a commercial method for the determination of metallothionein at the sensitivity levels required under the final cadmium rule is not currently available; therefore, analysis of CDU is recommended.
Among the general population not occupationally exposed to cadmium, CDU levels average less than 1 ?g/l (see Section 5.2.7). Normalized for creatinine (CRTU), the average CDU concentration of the general population is less than 1 ?g/g CRTU. As cadmium accumulates over the lifespan, CDU increases with age. Also, cigarette smokers may eventually accumulate twice the cadmium body burden of nonsmokers, CDU is slightly higher in smokers than in nonsmokers, even several years after smoking cessation (Nordberg and Nordberg 1988). Despite variations due to age and smoking habits, 95% of those not occupationally exposed to cadmium exhibit levels of CDU less than 3 ?g/g CRTU (based on the data presented in Section 5.2.7).
About 0.02% of the cadmium body burden is excreted daily in urine. When the critical cadmium concentration (about 200 ppm) in the kidney is reached, or if there is sufficient cadmium-induced kidney dysfunction, dramatic increases in CDU are observed (Nordberg and Nordberg 1988). Above 200 ppm, therefore, CDU concentrations cease to be an indicator of cadmium body burden, and are instead an index of kidney failure.
Proteinuria is an index of kidney dysfunction, and is defined by OSHA to be a material impairment. Several small proteins may be monitored as markers for proteinuria. Below levels indicative of proteinuria, these small proteins may be early indicators of increased risk of cadmium-induced renal tubular disease. Analytes useful for monitoring cadmium-induced renal tubular damage include:
1. ?-2-Microglobulin (B2M), currently the most widely used assay for detecting kidney dysfunction, is the best characterized analyte available (Iwao et al. 1980; Chia et al. 1989);
2. Retinol Binding Protein (RBP) is more stable than B2M in acidic urine (i.e., B2M breakdown occurs if urinary pH is less than 5.5; such breakdown may result in false [i.e., low] B2M values [Bernard and Lauw-erys, 1990]);
3. N-Acetyl-B-Glucosaminidase (NAG) is the analyte of an assay that is simple, inexpensive, reliable, and correlates with cadmium levels under 10 ?g/g CRTU, but the assay is less sensitive than RBP or B2M (Kawada et al. 1989);
4. Metallothionein (MT) correlates with cadmium and B2M levels, and may be a better predictor of cadmium exposure than CDU and B2M (Kawada et al. 1989);
5. Tamm-Horsfall Glycoprotein (THG) increases slightly with elevated cadmium levels, but this elevation is small compared to increases in urinary albumin, RBP, or B2M (Bernard and Lauwerys 1990);
6. Albumin (ALB), determined by the biuret method, is not sufficiently sensitive to serve as an early indicator of the onset of renal disease (Pis-cator 1962);
7. Albumin (ALB), determined by the Amido Black method, is sensitive and reproducible, but involves a time-consuming procedure (Piscator 1962);
8. Glycosaminoglycan (GAG) increases among cadmium workers, but the significance of this effect is unknown because no relationship has been found between elevated GAG and other indices of tubular damage (Bernard and Lauwerys 1990);
9. Trehalase seems to increase earlier than B2M during cadmium exposure, but the procedure for analysis is complicated and unreliable (Iwata et al. 1988); and,
10. Kallikrein is observed at lower concentrations among cadmium-exposed workers than among normal controls (Roels et al. 1990).
Of the above analytes, B2M appears to be the most widely used and best characterized analyte to evaluate the presence/absence, as well as the extent of, cadmium-induced renal tubular damage (Kawada, Koyama, and Suzuki 1989; Shaikh and Smith 1984; Nogawa 1984). However, it is important that samples be collected and handled so as to minimize B2M degradation under acidic urine conditions.
The threshold value of B2MU commonly used to indicate the presence of kidney damage 300 ?g/g CRTU (Kjellstrom et al. 1977a; Buchet et al. 1980; and Kowal and Zirkes 1983). This value represents the upper 95th or 97.5th percentile level of urinary excretion observed among those without tubular dysfunction (Elinder, exbt L-140-45, OSHA docket H057A). In agreement with these conclusions, the data presented in Section 5.3.7 of this protocol generally indicate that the level of 300 ?g/g CRTU appears to define the boundary for kidney dysfunction. It is not clear, however, that this level represents the upper 95th percentile of values observed among those who fail to demonstrate proteinuria effects.
Although elevated B2MU levels appear to be a fairly specific indicator of disease associated with cadmium exposure, other conditions that may lead to elevated B2MU levels include high fevers from influenza, extensive physical exercise, renal disease unrelated to cadmium exposure, lymphomas, and AIDS (Iwao et al. 1980; Schardun and van Epps 1987). Elevated B2M levels observed in association with high fevers from influenza or from extensive physical exercise are transient, and will return to normal levels once the fever has abated or metabolic rates return to baseline values following exercise. The other conditions linked to elevated B2M levels can be diagnosed as part of a properly-designed medical examination. Consequently, monitoring B2M, when accompanied by regular medical examinations and CDB and CDU determinations (as indicators of present and past cadmium exposure), may serve as a specific, early indicator of cadmium-induced kidney damage.
4.4 Criteria for Medical Monitoring of Cadmium Workers
Medical monitoring mandated by the final cadmium rule includes a combination of regular medical examinations and periodic monitoring of 3 analytes: CDB, CDU and B2MU. As indicated above, CDB is monitored as an indicator of current cadmium exposure, while CDU serves as an indicator of the cadmium body burden; B2MU is assessed as an early marker of irreversible kidney damage and disease.
The final cadmium rule defines a series of action levels that have been developed for each of the 3 analytes to be monitored. These action levels serve to guide the responsible physician through a decision-making process. For each action level that is exceeded, a specific response is mandated. The sequence of action levels, and the attendant actions, are described in detail in the final cadmium rule.
Other criteria used in the medical decision-making process relate to tests performed during the medical examination (including a determination of the ability of a worker to wear a respirator). These criteria, however, are not affected by the results of the analyte, determinations addressed in the above Paragraphs and, consequently, will not be considered further in these guidelines.
4.5 Defining to Quality and Proficiency of the Analyte Determinations
As noted above in Sections 2 and 3, the quality of a measurement should be defined along with its value to properly interpret the results. Generally, it is necessary to know the accuracy and the precision of a measurement before it can be properly evaluated. The precision of the data from a specific laboratory indicates the extent to which the repeated measurements of the same sample vary within that laboratory. The accuracy of the data provides an indication of the extent to which these results deviate from average results determined from many laboratories performing the same measurement (i.e., in the absence of an independent determination of the true value of a measurement). Note that terms are defined operationally relative to the manner in which they will be used in this protocol. Formal definitions for the terms in italics used in this section can be found in the list of definitions (Section 2).
Another data quality criterion required to properly evaluate measurement results is the limit of detection of that measurement. For measurements to be useful, the range of the measurement which is of interest for biological monitoring purposes must lie entirely above the limit of detection defined for that measurement.
The overall quality of a laboratory�s results is termed the performance of that laboratory. The degree to which a laboratory satisfies a minimum performance level is referred to as the proficiency of the laboratory. A successful medical monitoring program, therefore, should include procedures developed for monitoring and recording laboratory performance; these procedures can be used to identify the most proficient laboratories.
5.0 Overview of Medical Monitoring Tests for CDB, CDU, B2MU and CRTU
To evaluate whether available methods for assessing CDB, CDU, B2MU and CRTU are adequate for determining the parameters defined by the proposed action levels, it is necessary to review procedures available for sample collection, preparation and analysis. A variety of techniques for these purposes have been used historically for the determination of cadmium in biological matrices (including CDB and CDU), and for the determination of specific proteins in biological matrices (including B2MU). However, only the most recent techniques are capable of satisfying the required accuracy, precision and sensitivity (i.e., limit of detection) for monitoring at the levels mandated in the final cadmium rule, while still facilitating automated analysis and rapid processing.
5.1 Measuring Cadmium in Blood (CDB)
Analysis of biological samples for cadmium requires strict analytical discipline regarding collection and handling of samples. In addition to occupational settings, where cadmium contamination would be apparent, cadmium is a ubiquitous environmental contaminant, and much care should be exercised to ensure that samples are not contaminated during collection, preparation or analysis. Many common chemical reagents are contaminated with cadmium at concentrations that will interfere with cadmium analysis; because of the widespread use of cadmium compounds as colored pigments in plastics and coatings, the analyst should continually monitor each manufacturer�s chemical reagents and collection containers to prevent contamination of samples.
Guarding against cadmium contamination of biological samples is particularly important when analyzing blood samples because cadmium concentrations in blood samples from nonexposed populations are generally less than 2 ?g/l (2 ng/ml), while occupationally-exposed workers can be at medical risk to cadmium toxicity if blood concentrations exceed 5 ?g/l (ACGIH 1991 and 1992). This narrow margin between exposed and unexposed samples requires that exceptional care be used in performing analytic determinations for biological monitoring for occupational cadmium exposure.
Methods for quantifying cadmium in blood have improved over the last 40 years primarily because of improvements in analytical instrumentation. Also, due to improvements in analytical techniques, there is less need to perform extensive multi-step sample preparations prior to analysis. Complex sample preparation was previously required to enhance method sensitivity (for cadmium), and to reduce interference by other metals or components of the sample.
5.1.1 Analytical Techniques Used to Monitor Cadmium in Biological Matrices
| Analytical procedure | Limit of detection [ng/(g or ml)] | Specified biological matrix | Reference | Comments |
|---|---|---|---|---|
| Flame Atomic Absorption Spectroscopy (FAAS) | ?1.0 | Any matrix | Perkin-Elmer (1982) | Not sensitive enough for biomonitoring without extensive sample digestion, metal chelation and organic solvent extraction. |
| Graphite Furnace Atomic Absorption Spectroscopy (GFAAS) | 0.04 | Urine | Pruszkowska et al. (1983) | Methods of choice for routine cadmium analysis. |
| ?0.20 | Blood | Stoeppler and Brandt (1980). | ||
| Inductively-Coupled Argon-Plasma Atomic Emission Spectroscopy (ICAP AES) | 2.0 | Any matrix | NIOSH (1984A) | Requires extensive sample preparation and concentration of metal with chelating resin. Advantage is simultaneous analyses for as many as 10 metals from 1 sample. |
| Neutron Activation Gamma Spectroscopy (NA) | 1.5 | In vivo (liver). | Ellis et al. (1983) | Only available in vivo method for direct determination of cadmium body tissue burdens; expensive; absolute determination of cadmium in reference materials. |
| Isotope Dilution Mass Spectroscopy (IDMS) | <1.0 | Any matrix | Michiels and DeBievre (1986) | Suitable for absolute determination of cadmium in reference materials; expensive. |
| Differential Pulse Anodic Stripping Voltammetry (DPASV) | <1.0 | Any matrix | Stoeppler and Brandt (1980) | Suitable for absolute determination of cadmium in reference materials; efficient method to check accuracy of analytical method. |
A number of analytical techniques have been used for determining cadmium concentrations in biological materials. A summary of the characteristics of the most widely employed techniques is presented in Table 3. The technique most suitable for medical monitoring for cadmium is atomic absorption spectroscopy (AAS).
To obtain a measurement using AAS, a light source (i.e., hollow cathode or lectrode-free discharge lamp) containing the element of interest as the cathode, is energized and the lamp emits a spectrum that is unique for that element. This light source is focused through a sample cell, and a selected wavelength is monitored by a monochrometer and photodetector cell. Any ground state atoms in the sample that match those of the lamp element and are in the path of the emitted light may absorb some of the light and decrease the amount of light that reaches the photodetector cell. The amount of light absorbed at each characteristic wavelength is proportional to the number of ground state atoms of the corresponding element that are in the pathway of the light between the source and detector.
To determine the amount of a specific metallic element in a sample using AAS, the sample is dissolved in a solvent and aspirated into a high-temperature flame as an aerosol. At high temperatures, the solvent is rapidly evaporated or decomposed and the solute is initially solidified; the majority of the sample elements then are transformed into an atomic vapor. Next, a light beam is focused above the flame and the amount of metal in the sample can be determined by measuring the degree of absorbance of the atoms of the target element released by the flame at a characteristic wavelength.
A more refined atomic absorption technique, flameless AAS, substitutes an electrothermal, graphite furnace for the flame. An aliquot (10-100 ?l) of the sample is pipetted into the cold furnace, which is then heated rapidly to generate an atomic vapor of the element.
AAS is a sensitive and specific method for the elemental analysis of metals; its main drawback is nonspecific background absorbtion and scattering of the light beam by particles of the sample as it decomposes at high temperatures; nonspecific absorbance reduces the sensitivity of the analytical method. The problem of nonspecific absorbance and scattering can be reduced by extensive sample pretreatment, such as ashing and/or acid digestion of the sample to reduce its organic content.
Current AAS instruments employ background correction devices to adjust electronically for background absorbtion and scattering. A common method to correct for background effects is to use a deuterium arc lamp as a second light source. A continuum light source, such as the deuterium lamp, emits a broad spectrum of wavelengths instead of specific wavelengths characteristic of a particular element, as with the hollow cathode tube. With this system, light from the primary source and the continuum source are passed alternately through the sample cell. The target element effectively absorbs light only from the primary source (which is much brighter than the continuum source at the characteristic wavelengths), while the background matrix absorbs and scatters light from both sources equally. Therefore, when the ratio of the two beams is measured electronically, the effect of nonspecific background absorption and scattering is eliminated. A less common, but more sophisticated, background correction system is based on the Zeeman effect, which uses a magnetically-activated light polarizer to compensate electronically for nonspecific absorbtion and scattering.
Atomic emission spectroscopy with inductively-coupled argon plasma (AES-ICAP) is widely used to analyze for metals. With this instrument, the sample is aspirated into an extremely hot argon plasma flame, which excites the metal atoms; emission spectra specific for the sample element then are generated. The quanta of emitted light passing through a monochrometer are amplified by photomultiplier tubes and measured by a photodetector to determine the amount of metal in the sample. An advantage of AES-ICAP over AAS is that multi-elemental analyses of a sample can be performed by simultaneously measuring specific elemental emission energies. However, AES-ICAP lacks the sensitivity of AAS, exhibiting a limit of detection which is higher than the limit of detection for graphite-furnace AAS (Table 3).
Neutron activation (NA) analysis and isotope dilution mass spectrometry (IDMS) are 2 additional, but highly specialized, methods that have been used for cadmium determinations. These methods are expensive because they require elaborate and sophisticated instrumentation.
NA analysis has the distinct advantage over other analytical methods of being able to determine cadmium body burdens in specific organs (e.g., liver, kidney) in vivo (Ellis et al. 1983). Neutron bombardment of the target transforms cadmium-13 to cadmium-114, which promptly decays (<10 -14 sec) to its ground state, emitting gamma rays that are measured using large gamma detectors; appropriate shielding and instrumentation are required when using this method.
IDMS analysis, a definitive but laborious method, is based on the change in the ratio of 2 isotopes of cadmium (cadmium 111 and 112) that occurs when a known amount of the element (with an artificially altered ratio of the same isotopes [i.e., a cadmium 111 �spike�] is added to a weighed aliquot of the sample (Michiels and De Bievre 1986).
5.1.2 Methods Developed for CDB Determinations
A variety of methods have been used for preparing and analyzing CDB samples; most of these methods rely on one of the analytical techniques described above. Among the earliest reports, Princi (1947) and Smith et al. (1955) employed a colorimetric procedure to analyze for CDB and CDU. Samples were dried and digested through several cycles with concentrated mineral acids (HNO 3 and H 2 SO 4 ) and hydrogen peroxide(H 2 O 2 ). The digest was neutralized, and the cadmium was complexed with diphenylthiocarbazone and extracted with chloroform. The dithizone-cadmium complex then was quantified using a spectrometer.
Colorimetric procedures for cadmium analyses were replaced by methods based on atomic absorption spectroscopy (AAS) in the early 1960s, but many of the complex sample preparation procedures were retained. Kjellstrom (1979) reports that in Japanese, American and Swedish laboratories during the early 1970s, blood samples were wet ashed with mineral acids or ashed at high temperature and wetted with nitric acid. The cadmium in the digest was complexed with metal chelators including diethyl dithiocarbamate (DDTC), ammonium pyrrolidine dithiocarbamate (APDC) or diphenylthiocarbazone (dithizone) in ammonia-citrate buffer and extracted with methyl isobutyl ketone (MIBK). The resulting solution then was analyzed by flame AAS or graphite-furnace AAS for cadmium determinations using deuterium-lamp background correction.
In the late 1970s, researchers began developing simpler preparation procedures. Roels et al. (1978) and Roberts and Clark (1986) developed simplified digestion procedures. Using the Roberts and Clark method, a 0.5 ml aliquot of blood is collected and transferred to a digestion tube containing 1 ml concentrated HNO 3. The blood is then digested at 110�C for 4 hours. The sample is reduced in volume by continued heating, and 0.5 ml 30% H 2 O 2 is added as the sample dries. The residue is dissolved in 5 ml dilute (1%) HNO 3, and 20 ?l of sample is then analyzed by graphite-furnace AAS with deuterium-background correction.
The current trend in the preparation of blood samples is to dilute the sample and add matrix modifiers to reduce background interference, rather than digesting the sample to reduce organic content. The method of Stoeppler and Brandt (1980), and the abbreviated procedure published in the American Public Health Association�s (APHA) Methods for Biological Monitoring (1988), are straightforward and are nearly identical. For the APHA method, a small aliquot (50-300 ?l) of whole blood that has been stabilized with ethylenediaminetetraacetate (EDTA) is added to 1.0 ml 1MHNO 3, vigorously shaken and centrifuged. Aliquots (10-25 ?l) of the supernatant are then analyzed by graphite-furnace AAS with appropriate background correction.
Using the method of Stoeppler and Brandt (1980), aliquots (50-200 ?l) of whole blood that have been stabilized with EDTA are pipetted into clean polystyrene tubes and mixed with 150-600 ?l of 1 M HNO 3. After vigorous shaking, the solution is centrifuged and a 10-25 ?l aliquot of the supernatant then is analyzed by graphite-furnace AAS with appropriate background correction.
Claeys-Thoreau (1982) and DeBenzo et al. (1990) diluted blood samples at a ratio of 1:10 with a matrix modifier (0.2% Triton X-100, a wetting agent) for direct determinations of CDB. DeBenzo et al. also demonstrated that aqueous standards of cadmium, instead of spiked, whole-blood samples, could be used to establish calibration curves if standards and samples are treated with additional small volumes of matrix modifiers (i.e., 1% HNO 3, 0.2% ammonium hydrogenphosphate and 1 mg/ml magnesium salts).
These direct dilution procedures for CDB analysis are simple and rapid. Laboratories can process more than 100 samples a day using a dedicated graphite-furnace AAS, an auto-sampler, and either a Zeeman- or a deuterium-background correction system. Several authors emphasize using optimum settings for graphite-furnace temperatures during the drying, charring, and atomization processes associated with the flameless AAS method, and the need to run frequent QC samples when performing automated analysis.
5.1.3 Sample Collection and Handling
Sample collection procedures are addressed primarily to identify ways to minimize the degree of variability that may be introduced by sample collection during medical monitoring. It is unclear at this point the extent to which collection procedures contribute to variability among CDB samples. Sources of variation that may result from sampling procedures include time-of-day effects and introduction of external contamination during the collection process. To minimize these sources, strict adherence to a sample collection protocol is recommended. Such a protocol must include provisions for thorough cleaning of the site from which blood will be extracted; also, every effort should be made to collect samples near the same time of day. It is also important to recognize that under the recent OSHA blood-borne pathogens standard ( 29 CFR 1910.1030 ), blood samples and certain body fluids must be handled and treated as if they are infectious.
5.1.4 Best Achievable Performance
The best achievable performance using a particular method for CDB determinations is assumed to be equivalent to the performance reported by research laboratories in which the method was developed.
For their method, Roberts and Clark (1986) demonstrated a limit of detection of 0.4 ?g Cd/l in whole blood, with a linear response curve from 0.4 to 16.0 ?g Cd/l. They report a coefficient of variation (CV) of 6.7% at 8.0 ?g/l.
The APHA (1988) reports a range of 1.0-25 ?g/l, with a CV of 7.3% (concentration not stated). Insufficient documentation was available to critique this method.
Stoeppler and Brandt (1980) achieved a detection limit of 0.2 ?g Cd/l whole blood, with a linear range of 0.4-12.0 ?g Cd/l, and a CV of 15-30%, for samples at <1.0 ?g/l. Improved precision (CV of 3.8%) was reported for CDB concentrations at 9.3 ?g/l.
5.1.5 General Method Performance
For any particular method, the performance expected from commercial laboratories may be somewhat lower than that reported by the research laboratory in which the method was developed. With participation in appropriate proficiency programs and use of a proper in-house QA/QC program incorporating provisions for regular corrective actions, the performance of commercial laboratories is expected to approach that reported by research laboratories. Also, the results reported for existing proficiency programs serve as a gauge of the likely level of performance that currently can be expected from commercial laboratories offering these analyses.
Weber (1988) reports on the results of the proficiency program run by the Centre de Toxicologie du Quebec (CTQ). As indicated previously, participants in that program receive 18 blood samples per year having cadmium concentrations ranging from 0.2-20 ?g/l. Currently, 76 laboratories are participating in this program. The program is established for several analytes in addition to cadmium, and not all of these laboratories participate in the cadmium proficiency-testing program.
Under the CTQ program, cadmium results from individual laboratories are compared against the consensus mean derived for each sample. Results indicate that after receiving 60 samples (i.e., after participation for approximately three years), 60% of the laboratories in the program are able to report results that fall within � 1 ?g/l or 15% of the mean, whichever is greater. (For this procedure, the 15% criterion was applied to concentrations exceeding 7 ?g/l.) On any single sample of the last 20 samples, the percentage of laboratories falling within the specified range is between 55 and 80%.
The CTQ also evaluates the performance of participating laboratories against a less severe standard: � 2 ?g/l or 15% of the mean, whichever is greater (Weber 1988); 90% of participating laboratories are able to satisfy this standard after approximately 3 years in the program. (The 15% criterion is used for concentrations in excess of 13 ?g/l.) On any single sample of the last 15 samples, the percentage of laboratories falling within the specified range is between 80 and 95% (except for a single test for which only 60% of the laboratories achieved the desired performance).
Based on the data presented in Weber (1988), the CV for analysis of CDB is nearly constant at 20% for cadmium concentrations exceeding 5 ?g/l, and increases for cadmium concentrations below 5 ?g/l. At 2 ?g/l, the reported CV rises to approximately 40%. At 1 ?g/l, the reported CV is approximately 60%.
Participating laboratories also tend to overestimate concentrations for samples exhibiting concentrations less than 2 ?g/l (see Figure 11 of Weber 1988). This problem is due in part to the proficiency evaluation criterion that allows reporting a minimum � 2.0 ?g/l for evaluated CDB samples. There is currently little economic or regulatory incentive for laboratories participating in the CTQ program to achieve greater accuracy for CDB samples containing cadmium at concentrations less than 2.0 ?g/l, even if the laboratory has the experience and competency to distinguish among lower concentrations in the samples obtained from the CTQ.
The collective experience of international agencies and investigators demonstrate the need for a vigorous QC program to ensure that CDB values reported by participating laboratories are indeed reasonably accurate. As Friberg (1988) stated:
�Information about the quality of published data has often been lacking. This is of concern as assessment of metals in trace concentrations in biological media are fraught with difficulties from the collection, handling, and storage of samples to the chemical analyses. This has been proven over and over again from the results of interlaboratory testing and quality control exercises. Large variations in results were reported even from �experienced� laboratories.�
The UNEP/WHO global study of cadmium biological monitoring set a limit for CDB accuracy using the maximum allowable deviation method at Y=X � (0.1X+1) for a targeted concentration of 10 ?g Cd/l (Friberg and Vahter 1983). The performance of participating laboratories over a concentration range of 1.5-12 ?g/l was reported by Lind et al. (1987). Of the 3 QC runs conducted during 1982 and 1983, 1 or 2 of the 6 laboratories failed each run. For the years 1983 and 1985, between zero and 2 laboratories failed each of the consecutive QC runs.
In another study (Vahter and Friberg 1988), QC samples consisting of both external (unknown) and internal (stated) concentrations were distributed to laboratories participating in the epidemiology research. In this study, the maximum acceptable deviation between the regression analysis of reported results and reference values was set at Y=X � (0.05X+0.2) for a concentration range of 0.3-5.0 ?g Cd/l. It is reported that only 2 of 5 laboratories had acceptable data after the first QC set, and only 1 of 5 laboratories had acceptable data after the second QC set. By the fourth QC set, however, all 5 laboratories were judged proficient.
The need for high quality CDB monitoring is apparent when the toxicological and biological characteristics of this metal are considered; an increase in CDB from 2 to 4 ?g/l could cause a doubling of the cadmium accumulation in the kidney, a critical target tissue for selective cadmium accumulation (Nordberg and Nordberg 1988).
Historically, the CDC's internal QC program for CDB cadmium monitoring program has found achievable accuracy to be � 10% of the true value at CDB concentrations ?5.0 ?g/l (Paschal 1990). Data on the performance of laboratories participating in this program currently are not available.
5.1.6 Observed CDB Concentrations
As stated in Section 4.3, CDB concentrations are representative of ongoing levels of exposure to cadmium. Among those who have been exposed chronically to cadmium for extended periods, however, CDB may contain a component attributable to the general cadmium body burden.
5.1.6.1 CDB Concentrations Among Unexposed Samples
Numerous studies have been conducted examining CDB concentrations in the general population, and in control groups used for comparison with cadmium-exposed workers. A number of reports have been published that present erroneously high values of CDB (Nordberg and Nordberg 1988). This problem was due to contamination of samples during sampling and analysis, and to errors in analysis. Early AAS methods were not sufficiently sensitive to accurately estimate CDB concentrations.
Table 4 presents results of recent studies reporting CDB levels for the general U.S. population not exposed occupationally to cadmium. Other surveys of tissue cadmium using U.S. samples and conducted as part of a cooperative effort among Japan, Sweden and the U.S., did not collect CDB data because standard analytical methodologies were unavailable, and because of analytic problems (Kjellstrom 1979; SWRI 1978).
| Study No. | No. in Study (n) | Sex | Age | Smoking Habits b | Arithmetic mean (�S.D.) c | Absolute range or (95% CI) d | Geometric mean (GSD) e | Lower 95th percentile of distribution f | Upper 95th percentile of distribution f | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 80 | M | 4 to 69 | NS,S | 1.13 | 0.35�3.3 | 0.98�1.71 | 0.4 | 2.4 | Kowal et al. (1979). |
| 88 | F | 4 to 69 | NS,S | 1.03 | 0.21�3.3 | 0.91�1.63 | 0.4 | 2.0 | ||
| 115 | M/F | 4 to 69 | NS | 0.95 | 0.21�3.3 | 0.85�1.59 | 0.4 | 1.8 | ||
| 31 | M/F | 4 to 69 | S | 1.54 | 0.4�3.3 | 1.37�1.65 | 0.6 | 3.2 | ||
| 2 | 10 | M | Adults | (?) | 2.0�2.1 | (0.5�5.0) | g (0) | g (5.8) | Ellis et al. (1983). | |
| 3 | 24 | M | Adults | NS | 0.6� 1/87 | 0.2 | 1.8 | Frieberg and Vahter (1983). | ||
| 20 | M | Adults | S | 1.2�2.13 | 0.3 | 4.4 | ||||
| 64 | F | Adults | NS | 0.5�1.85 | 0.2 | 1.4 | ||||
| 39 | F | Adults | S | 0.8�2.22 | 0.2 | 3.1 | ||||
| 4 | 32 | M | Adults | S,NS | 1.2�2.0 | 0.4 | 3.9 | Thun et al. (1989). | ||
| 5 | 35 | M | Adults | (?) | 2.1�2.1 | (0.5�7.3) | g (0) | g (5.6) | Mueller et al. (1989). | |
| a Concentrations reported in ?g Cd/l blood unless otherwise stated | ||||||||||
| b NS-never smoked; S-current cigarette smoker | ||||||||||
| c S.D.-Arithmetic Standard Deviation. | ||||||||||
| d C.I.-Confidence Interval. | ||||||||||
| e GSD-Geometric Standard Deviation. | ||||||||||
| f Based on an assumed log normal distribution. | ||||||||||
| g Based on an assumed normal distribution. | ||||||||||
Arithmetic and/or geometric means and standard deviations are provided in Table 4 for measurements among the populations defined in each study listed. The range of reported measurements and/or the 95% upper and lower confidence intervals for the means are presented when this information was reported in a study. For studies reporting either an arithmetic or geometric standard deviation along with a mean, the lower and upper 95th percentile for the distribution also were derived and reported in the table.
The data provided in Table 4 from Kowal et al. (1979) are from studies conducted between 1974 and 1976 evaluating CDB levels for the general population in Chicago, and are considered to be representative of the U.S. population. These studies indicate that the average CDB concentration among those not occupationally exposed to cadmium is approximately 1 ?g/l.
In several other studies presented in Table 4, measurements are reported separately for males and females, and for smokers and nonsmokers. The data in this table indicate that similar CDB levels are observed among males and females in the general population, but that smokers tend to exhibit higher CDB levels than nonsmokers. Based on the Kowal et al. (1979) study, smokers not occupationally exposed to cadmium exhibit an average CDB level of 1.4 ?g/l.
In general, nonsmokers tend to exhibit levels ranging to 2 ?g/l, while levels observed among smokers range to 5 ?g/l. Based on the data presented in Table 4, 95% of those not occupationally exposed to cadmium exhibit CDB levels less than 5 ?g/l.
5.1.6.2 CDB Concentrations Among Exposed Workers
Table 5 is a summary of results from studies reporting CDB levels among workers exposed to cadmium in the work place. As in Table 4, arithmetic and/or geometric means and standard deviations are provided if reported in the listed studies. The absolute range, or the 95% confidence interval around the mean, of the data in each study are provided when reported. In addition, the lower and upper 95th percentile of the distribution are presented for each study in which a mean and corresponding standard deviation were reported. Table 5 also provides estimates of the duration, and level, of exposure to cadmium in the work place if these data were reported in the listed studies. The data presented in Table 5 suggest that CDB levels are dose related. Sukuri et al. (1983) show that higher CDB levels are observed among workers experiencing higher work place exposure. This trend appears to be true of every one of the studies listed in the table.
CDB levels reported in Table 5 are higher among those showing signs of cadmium-related kidney damage than those showing no such damage. Lauwerys et al. (1976) report CDB levels among workers with kidney lesions that generally are above the levels reported for workers without kidney lesions. Ellis et al. (1983) report a similar observation comparing workers with and without renal dysfunction, although they found more overlap between the 2 groups than Lauwerys et al.
| Study No. | Work environment (worker population monitored) | Number in study | Employment in years (mean) | Mean concentration of cadmium in air (?g/m 3 ) | Concentration of Cadmium in blood a | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Arithmetic mean (� S.D.) b | Absolute range or (95% CI) c | Geometric mean (GSD) d | Lower 95th percentile of range e () f | Upper 95th percentile of range e () f | Reference | |||||
| 1 | Ni-Cd battery plant and Cd production plant: | 3�40 | ?90 | Lauwerys et al. (1976). | ||||||
| (Workers without kidney lesions). | 96 | 21.4�1.9 | (18) | (25) | ||||||
| (Workers with kidney lesions). | 25 | 38.8�3.8 | (32) | (45) | ||||||
| 2 | Ni-Cd battery plant: | Adamsson et al. (1979). | ||||||||
| (Smokers) | 7 | (5) | 10.1 | 22.7 | 7.3�67.2 | |||||
| (Nonsmokers). | 8 | (9) | 7.0 | 7.0 | 4.9�10.5 | |||||
| 3 | Cadmium alloy plant: | Sukuri et al. (1982). | ||||||||
| (High exposure group). | 7 | (10.6) | [1,000-5 yrs; | 20.8�7.1 | (7.3) | (34) | ||||
| (Low exposure group). | 9 | (7.3) | 40-5 yrs] | 7.1�1.1 | (5.1) | (9.1) | ||||
| 4 | Retrospective study of workers with renal problems: | 19 | 15�41 | Roels et al. (1982). | ||||||
| (Before removal). | (27.2) | 39.9�3.7 | 11�179 | (34) | (46) | |||||
| (After removal). | (4.2) g | 14.1�5.6 | 5.7�27.4 | (4.4) | (24) | |||||
| 5 | Cadmium production plant: | Ellis et al. (1983). | ||||||||
| (Workers without renal dysfunction). | 33 | 1�34 | 15�5.7 | 7�31 | (5.4) | (25) | ||||
| (Workers with renal dysfunction). | 18 | 10�34 | 24�8.5 | 10�34 | (9.3) | (39) | ||||
| 6 | Cd-Cu alloy plant. | 75 | Up to 39 | 8.8�1.1 | 7.5 | 10 | Mason et al. (1988). | |||
| 7 | Cadmium recovery operation�Current (19) and former (26) workers. | 45 | (19.0) | 7.9�2.0 | 2.5 | 25 | Thun et al. (1989). | |||
| 8 | Cadmium recovery operation. | 40 | 10.2�5.3 | 2.2�18.8 | (1.3) | (19) | Mueller et al. (1989). | |||
| a Concentrations reported in ?g cd/l blood unless otherwise stated. | ||||||||||
| b S.D.-Standard Deviation. | ||||||||||
| c C.I.-Confidence Interval. | ||||||||||
| d GSD-Geometric Standard Deviation. | ||||||||||
| e Based on an assumed log normal distribution. | ||||||||||
| f Based on an assumed normal distribution. | ||||||||||
| g Years following removal. | ||||||||||
The data in Table 5 also indicate that CDB levels are higher among those experiencing current occupational exposure than those who have been removed from such exposure. Roels et al. (1982) indicate that CDB levels observed among workers experiencing ongoing exposure in the work place are almost entirely above levels observed among workers removed from such exposure. This finding suggests that CDB levels decrease once cadmium exposure has ceased.
A comparison of the data presented in Tables 4 and 5 indicates that CDB levels observed among cadmium-exposed workers is significantly higher than levels observed among the unexposed groups. With the exception of 2 studies presented in Table 5 (1 of which includes former workers in the sample group tested), the lower 95th percentile for CDB levels among exposed workers are greater than 5 ?g/l, which is the value of the upper 95th percentile for CDB levels observed among those who are not occupationally exposed. Therefore, a CDB level of 5 ?g/l represents a threshold above which significant work place exposure to cadmium may be occurring.
5.1.7 Conclusions and Recommendations for CDB
Based on the above evaluation, the following recommendations are made for a CDB proficiency program.
5.1.7.1 Recommended Method
The method of Stoeppler and Brandt (1980) should be adopted for analyzing CDB. This method was selected over other methods for its straightforward sample-preparation procedures, and because limitations of the method were described adequately. It also is the method used by a plurality of laboratories currently participating in the CTQ proficiency program. In a recent CTQ interlaboratory comparison report (CTQ 1991), analysis of the methods used by laboratories to measure CDB indicates that 46% (11 of 24) of the participating laboratories used the Stoeppler and Brandt methodology (HNO 3 deproteinization of blood followed by analysis of the supernatant by GF-AAS). Other CDB methods employed by participating laboratories identified in the CTQ report include dilution of blood (29%), acid digestion (12%) and miscellaneous methods (12%).
Laboratories may adopt alternate methods, but it is the responsibility of the laboratory to demonstrate that the alternate methods meet the data quality objectives defined for the Stoeppler and Brandt method (see section 5.1.7.2 below).
5.1.7.2 Data Quality Objectives
Based on the above evaluation, the following data quality objectives (DQOs) should facilitate interpretation of analytical results.
Limit of Detection. 0.5 ?g/l should be achievable using the Stoeppler and Brandt method. Stoeppler and Brandt (1980) report a limit of detection equivalent to 0.2 ?g/l in whole blood using 25 ?l aliquots of deproteinized, diluted blood samples.
Accuracy. Initially, some of the laboratories performing CDB measurements may be expected to satisfy criteria similar to the less severe criteria specified by the CTQ program, i.e., measurements within 2 ?g/l or 15% (whichever is greater) of the target value. About 60% of the laboratories enrolled in the CTQ program could meet this criterion on the first proficiency test (Weber 1988).
Currently, approximately 12 laboratories in the CTQ program are achieving an accuracy for CDB analysis within the more severe constraints of � 1 ?g/l or 15% (whichever is greater). Later, as laboratories gain experience, they should achieve the level of accuracy exhibited by these 12 laboratories. The experience in the CTQ program has shown that, even without incentives, laboratories benefit from the feedback of the program; after they have analyzed 40-50 control samples from the program, performance improves to the point where about 60% of the laboratories can meet the stricter criterion of � 1?g/l or 15% (Weber 1988). Thus, this stricter target accuracy is a reasonable DQO.
Precision. Although Stoeppler and Brandt (1980) suggest that a coefficient of variation (CV) near 1.3% (for a 10 ?g/l concentration) is achievable for within-run reproducibility, it is recognized that other factors affecting within- and between-run comparability will increase the achievable CV. Stoeppler and Brandt (1980) observed CVs that were as high as 30% for low concentrations (0.4 ?g/l), and CVs of less than 5% for higher concentrations.
For internal QC samples (see section 3.3.1), laboratories should to attain an overall precision near 25%. For CDB samples with concentrations less than 2 ?g/l, a target precision of 40% is reasonable, while precisions of 20% should be achievable for concentrations greater than 2 ?g/l. Although these values are more strict than values observed in the CTQ interlaboratory program reported by Weber (1988), they are within the achievable limits reported by Stoeppler and Brandt (1980).
5.1.7.3 Quality Assurance/Quality Control
Commercial laboratories providing measurement of CDB should adopt an internal QA/QC program that incorporates the following components: Strict adherence to the selected method, including all calibration requirements; regular incorporation of QC samples during actual runs; a protocol for corrective actions, and documentation of these actions; and, participation in an interlaboratory proficiency program. Note that the nonmandatory QA/QC program presented in Attachment 1 is based on the Stoeppler and Brandt method for CDB analysis. Should an alternate method be adopted, the laboratory should develop a QA/QC program satisfying the provisions of Section 3.3.1.
5.2 Measuring Cadmium in Urine (CDU)
As in the case of CDB measurement, proper determination of CDU requires strict analytical discipline regarding collection and handling of samples. Because cadmium is both ubiquitous in the environment and employed widely in coloring agents for industrial products that may be used during sample collection, preparation and analysis, care should be exercised to ensure that samples are not contaminated during the sampling procedure.
Methods for CDU determination share many of the same features as those employed for the determination of CDB. Thus, changes and improvements to methods for measuring CDU over the past 40 years parallel those used to monitor CDB. The direction of development has largely been toward the simplification of sample preparation techniques made possible because of improvements in analytic techniques.
5.2.1 Units of CDU Measurement
Procedures adopted for reporting CDU concentrations are not uniform. In fact, the situation for reporting CDU is more complicated than for CDB, where concentrations are normalized against a unit volume of whole blood.
Concentrations of solutes in urine vary with several biological factors (including the time since last voiding and the volume of liquid consumed over the last few hours); as a result, solute concentrations should be normalized against another characteristic of urine that represents changes in solute concentrations. The 2 most common techniques are either to standardize solute concentrations against the concentration of creatinine, or to standardize solute concentrations against the specific gravity of the urine. Thus, CDU concentrations have been reported in the literature as �uncorrected� concentrations of cadmium per volume of urine (i.e., ?g Cd/l urine), �corrected� concentrations of cadmium per volume of urine at a standard specific gravity (i.e., ?g Cd/l urine at a specific gravity of 1.020), or �corrected� mass concentration per unit mass of creatinine (i.e., ?g Cd/g creatinine). (CDU concentrations [whether uncorrected or corrected for specific gravity, or normalized to creatinine] occasionally are reported in nanomoles [i.e., nmoles] of cadmium per unit mass or volume. In this protocol, these values are converted to ?g of cadmium per unit mass or volume using 89 nmoles of cadmium=10 ?g.)
While it is agreed generally that urine values of analytes should be normalized for reporting purposes, some debate exists over what correction method should be used. The medical community has long favored normalization based on creatinine concentration, a common urinary constituent. Creatinine is a normal product of tissue catabolism, is excreted at a uniform rate, and the total amount excreted per day is constant on a day-to-day basis (NIOSH 1984b). While this correction method is accepted widely in Europe, and within some occupational health circles, Kowals (1983) argues that the use of specific gravity (i.e., total solids per unit volume) is more straightforward and practical (than creatinine) in adjusting CDU values for populations that vary by age or gender.
Kowals (1983) found that urinary creatinine (CRTU) is lower in females than males, and also varies with age. Creatinine excretion is highest in younger males (20-30 years old), decreases at middle age (50-60 years), and may rise slightly in later years. Thus, cadmium concentrations may be underestimated for some workers with high CRTU levels.
Within a single void urine collection, urine concentration of any analyte will be affected by recent consumption of large volumes of liquids, and by heavy physical labor in hot environments. The absolute amount of analyte excreted may be identical, but concentrations will vary widely so that urine must be corrected for specific gravity (i.e., to normalize concentrations to the quantity of total solute) using a fixed value (e.g., 1.020 or 1.024). However, since heavy-metal exposure may increase urinary protein excretion, there is a tendency to underestimate cadmium concentrations in samples with high specific gravities when specific-gravity corrections are applied.
Despite some shortcomings, reporting solute concentrations as a function of creatinine concentration is accepted generally; OSHA therefore recommends that CDU levels be reported as the mass of cadmium per unit mass of creatinine (?g/g CTRU).
Reporting CDU as ?g/g CRTU requires an additional analytical process beyond the analysis of cadmium: Samples must be analyzed independently for creatinine so that results may be reported as the ratio of cadmium to creatinine concentrations found in the urine sample. Consequently, the overall quality of the analysis depends on the combined performance by a laboratory on these 2 determinations. The analysis used for CDU determinations is addressed below in terms of ?g Cd/l, with analysis of creatinine addressed separately. Techniques for assessing creatinine are discussed in Section 5.4.
Techniques for deriving cadmium as a ratio of CRTU, and the confidence limits for independent measurements of cadmium and CRTU, are provided in Section 3.3.3.
5.2.2 Analytical Techniques Used to Monitor CDU
Analytical techniques used for CDU determinations are similar to those employed for CDB determinations; these techniques are summarized in Table 3. As with CDB monitoring, the technique most suitable for CDU determinations is atomic absorption spectroscopy (AAS). AAS methods used for CDU determinations typically employ a graphite furnace, with background correction made using either the deuterium-lamp or Zeeman techniques; Section 5.1.1 provides a detailed description of AAS methods.
5.2.3 Methods Developed for CDU Determinations
Princi (1947), Smith et al. (1955), Smith and Kench (1957), and Tsuchiya (1967) used colorimetric procedures similar to those described in the CDB section above to estimate CDU concentrations. In these methods, urine (50 ml) is reduced to dryness by heating in a sand bath and digested (wet ashed) with mineral acids. Cadmium then is complexed with dithiazone, extracted with chloroform and quantified by spectrophotometry. These early studies typically report reagent blank values equivalent to 0.3 ?g Cd/l, and CDU concentrations among nonexposed control groups at maximum levels of 10 ?g Cd/l�erroneously high values when compared to more recent surveys of cadmium concentrations in the general population.
By the mid-1970s, most analytical procedures for CDU analysis used either wet ashing (mineral acid) or high temperatures (>400� C) to digest the organic matrix of urine, followed by cadmium chelation with APDC or DDTC solutions and extraction with MIBK. The resulting aliquots were analyzed by flame or graphite-furnace AAS (Kjellstrom 1979).
Improvements in control over temperature parameters with electrothermal heating devices used in conjunction with flameless AAS techniques, and optimization of temperature programs for controlling the drying, charring, and atomization processes in sample analyses, led to improved analytical detection of diluted urine samples without the need for sample digestion or ashing. Roels et al. (1978) successfully used a simple sample preparation, dilution of 1.0 ml aliquots of urine with 0.1 N HNO 3, to achieve accurate low-level determinations of CDU.
In the method described by Pruszkowska et al. (1983), which has become the preferred method for CDU analysis, urine samples were diluted at a ratio of 1:5 with water; diammonium hydrogenphosphate in dilute HNO 3 was used as a matrix modifier. The matrix modifier allows for a higher charring temperature without loss of cadmium through volatilization during pre-atomization. This procedure also employs a stabilized temperature platform in a graphite furnace, while nonspecific background absorbtion is corrected using the Zeeman technique. This method allows for an absolute detection limit of approximately 0.04 ?g Cd/l urine.
5.2.4 Sample Collection and Handling
Sample collection procedures for CDU may contribute to variability observed among CDU measurements. Sources of variation attendant to sampling include time-of-day, the interval since ingestion of liquids, and the introduction of external contamination during the collection process. Therefore, to minimize contributions from these variables, strict adherence to a sample-collection protocol is recommended. This protocol should include provisions for normalizing the conditions under which urine is collected. Every effort also should be made to collect samples during the same time of day.
Collection of urine samples from an industrial work force for biological monitoring purposes usually is performed using �spot� (i.e., single-void) urine with the pH of the sample determined immediately. Logistic and sample-integrity problems arise when efforts are made to collect urine over long periods (e.g., 24 hrs). Unless single-void urines are used, there are numerous opportunities for measurement error because of poor control over sample collection, storage and environmental contamination.
To minimize the interval during which sample urine resides in the bladder, the following adaption to the �spot� collection procedure is recommended: The bladder should first be emptied, and then a large glass of water should be consumed; the sample may be collected within an hour after the water is consumed.
5.2.5 Best Achievable Performance
Performance using a particular method for CDU determinations is assumed to be equivalent to the performance reported by the research laboratories in which the method was developed. Pruszkowska et al. (1983) report a detection limit of 0.04 ?g/l CDU, with a CV of <4% between 0-5 ?g/l. The CDC reports a minimum CDU detection limit of 0.07 ?g/l using a modified method based on Pruszkowska et al. (1983). No CV is stated in this protocol; the protocol contains only rejection criteria for internal QC parameters used during accuracy determinations with known standards (Attachment 8 of exhibit 106 of OSHA docket H057A). Stoeppler and Brandt (1980) report a CDU detection limit of 0.2 ?g/l for their methodology.
5.2.6 General Method Performance
For any particular method, the expected initial performance from commercial laboratories may be somewhat lower than that reported by the research laboratory in which the method was developed. With participation in appropriate proficiency programs, and use of a proper in-house QA/QC program incorporating provisions for regular corrective actions, the performance of commercial laboratories may be expected to improve and approach that reported by a research laboratories. The results reported for existing proficiency programs serve to specify the initial level of performance that likely can be expected from commercial laboratories offering analysis using a particular method.
Weber (1988) reports on the results of the CTQ proficiency program, which includes CDU results for laboratories participating in the program. Results indicate that after receiving 60 samples (i.e., after participating in the program for approximately 3 years), approximately 80% of the participating laboratories report CDU results ranging between �2 ?g/l or 15% of the consensus mean, whichever is greater. On any single sample of the last 15 samples, the proportion of laboratories falling within the specified range is between 75 and 95%, except for a single test for which only 60% of the laboratories reported acceptable results. For each of the last 15 samples, approximately 60% of the laboratories reported results within � 1 ?g or 15% of the mean, whichever is greater. The range of concentrations included in this set of samples was not reported.
Another report from the CTQ (1991) summarizes preliminary CDU results from their 1991 interlaboratory program. According to the report, for 3 CDU samples with values of 9.0, 16.8, 31.5 ?g/l, acceptable results (target � 2 ?g/l or 15% of the consensus mean, whichever is greater) were achieved by only 44-52% of the 34 laboratories participating in the CDU program. The overall CVs for these 3 CDU samples among the 34 participating laboratories were 31%, 25%, and 49%, respectively. The reason for this poor performance has not been determined.
A more recent report from the CTQ (Weber, private communication) indicates that 36% of the laboratories in the program have been able to achieve the target of �1 ?g/l or 15% for more than 75% of the samples analyzed over the last 5 years, while 45% of participating laboratories achieved a target of �2 ?g/l or 15% for more than 75% of the samples analyzed over the same period.
Note that results reported in the interlaboratory programs are in terms of ?g Cd/l of urine, unadjusted for creatinine. The performance indicated, therefore, is a measure of the performance of the cadmium portion of the analyses, and does not include variation that may be introduced during the analysis of CRTU.
5.2.7 Observed CDU Concentrations
Prior to the onset of renal dysfunction, CDU concentrations provide a general indication of the exposure history (i.e., body burden) (see Section 4.3). Once renal dysfunction occurs, CDU levels appear to increase and are no longer indicative solely of cadmium body burden (Friberg and Elinder 1988).
5.2.7.1 Range of CDU Concentrations Observed Among Unexposed Samples
Surveys of CDU concentrations in the general population were first reported from cooperative studies among industrial countries (i.e., Japan, U.S. and Sweden) conducted in the mid-1970s. In summarizing these data, Kjellstrom (1979) reported that CDU concentrations among Dallas, Texas men (age range: <9-59 years; smokers and nonsmokers) varied from 0.11-1.12 ?g/l (uncorrected for creatinine or specific gravity). These CDU concentrations are intermediate between population values found in Sweden (range: 0.11-0.80 ?g/l) and Japan (range: 0.14-2.32 ?g/l).
Kowal and Zirkes (1983) reported CDU concentrations for almost 1,000 samples collected during 1978-79 from the general U.S. adult population (i.e., nine states; both genders; ages 20-74 years). They report that CDU concentrations are lognormally distributed; low levels predominated, but a small proportion of the population exhibited high levels. These investigators transformed the CDU concentrations values, and reported the same data 3 different ways: ?g/l urine (unadjusted), ?g/l (specific gravity adjusted to 1.020), and ?g/g CRTU. These data are summarized in Tables 6 and 7.
Based on further statistical examination of these data, including the lifestyle characteristics of this group, Kowal (1988) suggested increased cadmium absorption (i.e., body burden) was correlated with low dietary intakes of calcium and iron, as well as cigarette smoking.
CDU levels presented in Table 6 are adjusted for age and gender. Results suggest that CDU levels may be slightly different among men and women (i.e., higher among men when values are unadjusted, but lower among men when the values are adjusted, for specific gravity or CRTU). Mean differences among men and women are small compared to the standard deviations, and therefore may not be significant. Levels of CDU also appear to increase with age. The data in Table 6 suggest as well that reporting CDU levels adjusted for specific gravity or as a function of CRTU results in reduced variability.
| Geometric means (and geometric standard deviations) | |||
|---|---|---|---|
| Unadjusted (?g/l) | SG-adjusted 2 (?g/l at 1.020) | Creatine-adjusted (?g/g) | |
| Sex: | |||
| Male (n = 484) | 0.55 (2.9) | 0.73 (2.6) | 0.55 (2.7) |
| Female (n = 498) | 0.49 (3.0) | 0.86 (2.7) | 0.78 (2.7) |
| Age: | |||
| 20�29 (n = 222) | 0.32 (3.0) | 0.43 (2.7) | 0.32 (2.7) |
| 30�39 (n = 141) | 0.46 (3.2) | 0.70 (2.8) | 0.54 (2.7) |
| 40�49 (n = 142) | 0.50 (3.0) | 0.81 (2.6) | 0.70 (2.7) |
| 50�59 (n = 117) | 0.61 (2.9) | 0.99 (2.4) | 0.90 (2.3) |
| 60�69 (n = 272) | 0.76 (2.6) | 1.16 (2.3) | 1.03 (2.3) |
| 1 From Kowal and Zirkes 1983 | |||
| 2 SC-adjusted for specific gravity | |||
| Range of concentrations | Unadjusted (?g/l) | SG-adjusted (?g/l at 1.020) | Creatine-adjusted(?g/g) |
|---|---|---|---|
| <0.5 | 43.9 | 28.0 | 35.8 |
| 0.6�1.0 | 71.7 | 56.4 | 65.6 |
| 1.1�1.5 | 84.4 | 74.9 | 81.4 |
| 1.6�2.0 | 91.3 | 84.7 | 88.9 |
| 2.1�3.0 | 97.3 | 94.4 | 95.8 |
| 3.1�4.0 | 98.8 | 97.4 | 97.2 |
| 4.1�5.0 | 99.4 | 98.2 | 97.9 |
| 5.1�10.0 | 99.6 | 99.4 | 99.3 |
| 10.0�20.0 | 99.8 | 99.6 | 99.6 |
| 1 Source: Kowal and Zirkes (1983). | |||
The data in the Table 6 indicate the geometric mean of CDU levels observed among the general population is 0.52 ?g Cd/l urine (unadjusted), with a geometric standard deviation of 3.0. Normalized for creatinine, the geometric mean for the population is 0.66 ?g/g CRTU, with a geometric standard deviation of 2.7. Table 7 provides the distributions of CDU concentrations for the general population studied by Kowal and Zirkes. The data in this table indicate that 95% of the CDU levels observed among those not occupationally exposed to cadmium are below 3 ?g/g CRTU.
5.2.7.2 Range of CDU Concentrations Observed Among Exposed Workers
Table 8 is a summary of results from available studies of CDU concentrations observed among cadmium-exposed workers. In this table, arithmetic and/or geometric means and standard deviations are provided if reported in these studies. The absolute range for the data in each study, or the 95% confidence interval around the mean of each study, also are provided when reported. The lower and upper 95th percentile of the distribution are presented for each study in which a mean and corresponding standard deviation were reported. Table 8 also provides estimates of the years of exposure, and the levels of exposure, to cadmium in the work place if reported in these studies. Concentrations reported in this table are in ?g/g CRTU, unless otherwise stated.
| Study No. | Work environment (worker population monitored) | Number in study (n) | Employment in years (mean) | Mean concentration of cadmium in air (?g/m 3 ) | Concentrations of Cadmium in Urine a | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Arithmetic mean (�S.D.) b | Absolute range or (95% CI) c | Geometric mean (GSD) d | Lower 95th percentile of range e () f | Upper 95th percentile of range e () f | Reference | |||||
| 1 | Ni-Cd battery plant and Cd production plant. | 3�40 | ?90 | Lauwerys et al. 176. | ||||||
| (Workers without kidney lesions). | 96 | 16.3�16.7 | (0) | (44) | ||||||
| (Workers with kidney lesions). | 25 | 48.2�42.6 | (0) | (120) | ||||||
| 2 | Ni-Cd battery plant. | Adamsson et al. (1979). | ||||||||
| (Smokers)... | 7 | (5) | 10.1 | 5.5 | 1.0�14.7 | |||||
| (Nonsmokers). | 8 | (9) | 7.0 | 3.6 | 0.5�9.3 | |||||
| 3 | Cadmium salts production facility. | 148 | (15.4) | 15.8 | 2�150 | Butchet et al. 1980. | ||||
| 4 | Retrospective study of workers with renal problems. | 19 | 15�41 | Roels et al. 1982. | ||||||
| (Before removal). | (27.2) | 39.4�28.1 | 10.8�117 | (0) | (88) | |||||
| (After removal). | (4.2) g | 16.4�9.0 | 80�42.3 | (1.0) | (32) | |||||
| 5 | Cadmium production plant. | Ellis et al. 1983. | ||||||||
| (Workers without renal dysfunction). | 33 | 1�34 | 9.4�6.9 | 2�27 | (0) | (21) | ||||
| (Workers with renal dysfunction). | 18 | 10�34 | 22.8�12.7 | 8�55 | (1) | (45) | ||||
| 6 | Cd-Cu alloy plant. | 75 | Up to 39 | Note h | 6.9�9.4 | (0) | (23) | Mason et al. 1988. | ||
| 7 | Cadmium recovery operation. | 45 | (19) | 87 | 9.3�6.9 | (0) | (21) | Thun et al. 1989. | ||
| 8 | Pigment manufacturing plant. | 29 | (12.8) | 0.18�3.0 | 0.2�9.5 | 1.1 | Mueller et al. 1989. | |||
| 9 | Pigment manufacturing plant. | 26 | (12.1) | ?3.0 | 1.25�2.45 | 0.3 | 6 | Kawada et al. 1990. | ||
| a Concentrations are reported in ?g/g Cr. | ||||||||||
| b S.D.-Standard Deviation. | ||||||||||
| c C.I.-Confidence Interval. | ||||||||||
| d GSD-Geometric Standard Deviation | ||||||||||
| e Based on an assumed lognormal distribution. | ||||||||||
| f Based on an assumed normal distribution. | ||||||||||
| g Years following removal. | ||||||||||
| h Equivalent to 50 for 20�22 yrs. | ||||||||||
Data in Table 8 from Lauwerys et al. (1976) and Ellis et al. (1983) indicate that CDU concentrations are higher among those exhibiting kidney lesions or dysfunction than among those lacking these symptoms. Data from the study by Roels et al. (1982) indicate that CDU levels decrease among workers removed from occupational exposure to cadmium in comparison to workers experiencing ongoing exposure. In both cases, however, the distinction between the 2 groups is not as clear as with CDB; there is more overlap in CDU levels observed among each of the paired populations than is true for corresponding CDB levels. As with CDB levels, the data in Table 8 suggest increased CDU concentrations among workers who experienced increased overall exposure.
Although a few occupationally-exposed workers in the studies presented in Table 8 exhibit CDU levels below 3 ?g/g CRTU, most of those workers exposed to cadmium levels in excess of the PEL defined in the final cadmium rule exhibit CDU levels above 3 ?g/g CRTU; this level represents the upper 95th percentile of the CDU distribution observed among those who are not occupationally exposed to cadmium (Table 7).
The mean CDU levels reported in Table 8 among occupationally-exposed groups studied (except 2) exceed 3 ?g/g CRTU. Correspondingly, the level of exposure reported in these studies (with 1 exception) are significantly higher than what workers will experience under the final cadmium rule. The 2 exceptions are from the studies by Mueller et al. (1989) and Kawada et al. (1990); these studies indicate that workers exposed to cadmium during pigment manufacture do not exhibit CDU levels as high as those levels observed among workers exposed to cadmium in other occupations. Exposure levels, however, were lower in the pigment manufacturing plants studied. Significantly, workers removed from occupational cadmium exposure for an average of 4 years still exhibited CDU levels in excess of 3 ?g/g CRTU (Roels et al. 1982). In the single-exception study with a reported level of cadmium exposure lower than levels proposed in the final rule (i.e., the study of a pigment manufacturing plant by Kawada et al. 1990), most of the workers exhibited CDU levels less than 3 ?g/g CRTU (i.e., the mean value was only 1.3 ?g/g CRTU). CDU levels among workers with such limited cadmium exposure are expected to be significantly lower than levels of other studies reported on Table 8.
Based on the above data, a CDU level of 3 ?g/g CRTU appear to represent a threshold above which significant work place exposure to cadmium occurs over the work span of those being monitored. Note that this threshold is not as distinct as the corresponding threshold described for CDB. In general, the variability associated with CDU measurements among exposed workers appears to be higher than the variability associated with CDB measurements among similar workers.
5.2.8 Conclusions and Recommendations for CDU
The above evaluation supports the following recommendations for a CDU proficiency program. These recommendations address only sampling and analysis procedures for CDU determinations specifically, which are to be reported as an unadjusted ?g Cd/l urine. Normalizing this result to creatinine requires a second analysis for CRTU so that the ratio of the 2 measurements can be obtained. Creatinine analysis is addressed in Section 5.4. Formal procedures for combining the 2 measurements to derive a value and a confidence limit for CDU in ?g/g CRTU are provided in Section 3.3.3.
5.2.8.1 Recommended Method
The method of Pruszkowska et al. (1983) should be adopted for CDU analysis. This method is recommended because it is simple, straightforward and reliable (i.e., small variations in experimental conditions do not affect the analytical results).
A synopsis of the methods used by laboratories to determine CDU under the interlaboratory program administered by the CTQ (1991) indicates that more than 78% (24 of 31) of the participating laboratories use a dilution method to prepare urine samples for CDU analysis. Laboratories may adopt alternate methods, but it is the responsibility of the laboratory to demonstrate that the alternate methods provide results of comparable quality to the Pruszkowska method.
5.2.8.2 Data Quality Objectives
The following data quality objectives should facilitate interpretation of analytical results, and are achievable based on the above evaluation.
Limit of Detection. A level of 0.5 ?g/l (i.e., corresponding to a detection limit of 0.5 ?g/g CRTU, assuming 1 g CRT/l urine) should be achievable. Pruszkowska et al. (1983) achieved a limit of detection of 0.04 ?g/l for CDU based on the slope of the curve for their working standards (0.35 pg Cd/0.0044, A signal=1% absorbance using GF-AAS).
The CDC reports a minimum detection limit for CDU of 0.07 ?g/l using a modified Pruszkowska method. This limit of detection was defined as 3 times the standard deviation calculated from 10 repeated measurements of a �low level� CDU test sample (Attachment 8 of exhibit 106 of OSHA docket H057A).
Stoeppler and Brandt (1980) report a limit of detection for CDU of 0.2 ?g/l using an aqueous dilution (1:2) of the urine samples.
Accuracy. A recent report from the CTQ (Weber, private communication) indicates that 36% of the laboratories in the program achieve the target of �1 ?g/l or 15% for more than 75% of the samples analyzed over the last 5 years, while 45% of participating laboratories achieve a target of �2 ?g/l or 15% for more than 75% of the samples analyzed over the same period. With time and a strong incentive for improvement, it is expected that the proportion of laboratories successfully achieving the stricter level of accuracy should increase. It should be noted, however, these indices of performance do not include variations resulting from the ancillary measurement of CRTU (which is recommended for the proper recording of results). The low cadmium levels expected to be measured indicate that the analysis of creatinine will contribute relatively little to the overall variability observed among creatinine-normalized CDU levels (see Section 5.4). The initial target value for reporting CDU under this program, therefore, is set at �1 ?g/g CRTU or 15% (whichever is greater).
Precision. For internal QC samples (which are recommended as part of an internal QA/QC program, Section 3.3.1), laboratories should attain an overall precision of 25%. For CDB samples with concentrations less than 2 ?g/l, a target precision of 40% is acceptable, while precisions of 20% should be achievable for CDU concentrations greater than 2 ?g/l. Although these values are more stringent than those observed in the CTQ interlaboratory program reported by Weber (1988), they are well within limits expected to be achievable for the method as reported by Stoeppler and Brandt (1980).
5.2.8.3 Quality Assurance/Quality Control
Commercial laboratories providing CDU determinations should adopt an internal QA/QC program that incorporates the following components: Strict adherence to the selected method, including calibration requirements; regular incorporation of QC samples during actual runs; a protocol for corrective actions, and documentation of such actions; and, participation in an interlaboratory proficiency program. Note that the nonmandatory program presented in Attachment 1 as an example of an acceptable QA/QC program, is based on using the Pruszkowska method for CDU analysis. Should an alternate method be adopted by a laboratory, the laboratory should develop a QA/QC program equivalent to the nonmandatory program, and which satisfies the provisions of Section 3.3.1.
5.3 Monitoring ?-2-Microglobulin in Urine (B2MU).
As indicated in Section 4.3, B2MU appears to be the best of several small proteins that may be monitored as early indicators of cadmium-induced renal damage. Several analytic techniques are available for measuring B2M.
5.3.1 Units of B2MU Measurement
Procedures adopted for reporting B2MU levels are not uniform. In these guidelines, OSHA recommends that B2MU levels be reported as ?g/g CRTU, similar to reporting CDU concentrations. Reporting B2MU normalized to the concentration of CRTU requires an additional analytical process beyond the analysis of B2M: Independent analysis for creatinine so that results may be reported as a ratio of the B2M and creatinine concentrations found in the urine sample. Consequently, the overall quality of the analysis depends on the combined performance on these 2 analyses. The analysis used for B2MU determinations is described in terms of ?g B2M/l urine, with analysis of creatinine addressed separately. Techniques used to measure creatinine are provided in Section 5.4. Note that Section 3.3.3 provides techniques for deriving the value of B2M as function of CRTU, and the confidence limits for independent measurements of B2M and CRTU.
5.3.2 Analytical Techniques Used to Monitor B2MU
One of the earliest tests used to measure B2MU was the radial immunodiffusion technique. This technique is a simple and specific method for identification and quantitation of a number of proteins found in human serum and other body fluids when the protein is not readily differentiated by standard electrophoretic procedures. A quantitative relationship exists between the concentration of a protein deposited in a well that is cut into a thin agarose layer containing the corresponding monospecific antiserum, and the distance that the resultant complex diffuses. The wells are filled with an unknown serum and the standard (or control), and incubated in a moist environment at room temperature. After the optimal point of diffusion has been reached, the diameters of the resulting precipition rings are measured. The diameter of a ring is related to the concentration of the constituent substance. For B2MU determinations required in the medical monitoring program, this method requires a process that may be insufficient to concentrate the protein to levels that are required for detection.
Radioimmunoassay (RIA) techniques are used widely in immunologic assays to measure the concentration of antigen or antibody in body-fluid samples. RIA procedures are based on competitive-binding techniques. If antigen concentration is being measured, the principle underlying the procedure is that radioactive-labeled antigen competes with the sample�s unlabeled antigen for binding sites on a known amount of immobile antibody. When these 3 components are present in the system, an equilibrium exists. This equilibrium is followed by a separation of the free and bound forms of the antigen. Either free or bound radioactive-labeled antigen can be assessed to determine the amount of antigen in the sample. The analysis is performed by measuring the level of radiation emitted either by the bound complex following removal of the solution containing the free antigen, or by the isolated solution containing the residual-free antigen. The main advantage of the RIA method is the extreme sensitivity of detection for emitted radiation and the corresponding ability to detect trace amounts of antigen. Additionally, large numbers of tests can be performed rapidly.
The enzyme-linked immunosorbent assay (ELISA) techniques are similar to RIA techniques except that nonradioactive labels are employed. This technique is safe, specific and rapid, and is nearly as sensitive as RIA techniques. An enzyme-labeled antigen is used in the immunologic assay; the labeled antigen detects the presence and quantity of unlabeled antigen in the sample. In a representative ELISA test, a plastic plate is coated with antibody (e.g., antibody to B2M). The antibody reacts with antigen (B2M) in the urine and forms an antigen-antibody complex on the plate. A second anti-B2M antibody (i.e., labeled with an enzyme) is added to the mixture and forms an antibody-antigen-antibody complex. Enzyme activity is measured spectrophotometrically after the addition of a specific chromogenic substrate which is activated by the bound enzyme. The results of a typical test are calculated by comparing the spectrophotometric reading of a serum sample to that of a control or reference serum. In general, these procedures are faster and require less laboratory work than other methods.
In a fluorescent ELISA technique (such as the one employed in the Pharmacia Delphia test for B2M), the labeled enzyme is bound to a strong fluorescent dye. In the Pharmacia Delphia test, an antigen bound to a fluorescent dye competes with unlabeled antigen in the sample for a predetermined amount of specific, immobile antibody. Once equilibrium is reached, the immobile phase is removed from the labeled antigen in the sample solution and washed; an enhancement solution then is added that liberates the fluorescent dye from the bound antigen-antibody complex. The enhancement solution also contains a chelate that complexes with the fluorescent dye in solution; this complex increases the fluorescent properties of the dye so that it is easier to detect.
To determine the quantity of B2M in a sample using the Pharmacia Delphia test, the intensity of the fluorescence of the enhancement solution is measured. This intensity is proportional to the concentration of labeled antigen that bound to the immobile antibody phase during the initial competition with unlabeled antigen from the sample. Consequently, the intensity of the fluorescence is an inverse function of the concentration of antigen (B2M) in the original sample. The relationship between the fluorescence level and the B2M concentration in the sample is determined using a series of graded standards, and extrapolating these standards to find the concentration of the unknown sample.
5.3.3 Methods Developed for B2MU Determinations
B2MU usually is measured by radioimmunoassay (RIA) or enzyme-linked immunosorbent assay (ELISA); however, other methods (including gel electrophoresis, radial immunodiffusion, and nephelometric assays) also have been described (Schardun and van Epps 1987). RIA and ELI-SA methods are preferred because they are sensitive at concentrations as low as micrograms per liter, require no concentration processes, are highly reliable and use only a small sample volume.
Based on a survey of the literature, the ELISA technique is recommended for monitoring B2MU. While RIAs provide greater sensitivity (typically about 1 ?g/l, Evrin et al. 1971), they depend on the use of radioisotopes; use of radioisotopes requires adherence to rules and regulations established by the Atomic Energy Commission, and necessitates an expensive radioactivity counter for testing. Radioisotopes also have a relatively short half-life, which corresponds to a reduced shelf life, thereby increasing the cost and complexity of testing. In contrast, ELISA testing can be performed on routine laboratory spectrophotometers, do not necessitate adherence to additional rules and regulations governing the handling of radioactive substances, and the test kits have long shelf lives. Further, the range of sensitivity commonly achieved by the recommended ELISA test (i.e., the Pharmacia Delphia test) is approximately 100 ?g/l (Pharmacia 1990), which is sufficient for monitoring B2MU levels resulting from cadmium exposure. Based on the studies listed in
Table 9 (Section 5.3.7), the average range of B2M concentrations among the general, non-exposed population falls between 60 and 300 ?g/g CRTU. The upper 95th percentile of distributions, derived from studies in Table 9 which reported standard deviations, range between 180 and 1,140 ?g/g CRTU. Also, the Pharmacia Delphia test currently is the most widely used test for assessing B2MU.
5.3.4 Sample Collection and Handling
As with CDB or CDU, sample collection procedures are addressed primarily to identify ways to minimize the degree of variability introduced by sample collection during medical monitoring. It is unclear the extent to which sample collection contributes to B2MU variability. Sources of variation include time-of-day effects, the interval since consuming liquids and the quantity of liquids consumed, and the introduction of external contamination during the collection process. A special problem unique to B2M sampling is the sensitivity of this protein to degradation under acid conditions commonly found in the bladder. To minimize this problem, strict adherence to a sampling protocol is recommended. The protocol should include provisions for normalizing the conditions under which the urine is collected. Clearly, it is important to minimize the interval urine spends in the bladder. It also is recommended that every effort be made to collect samples during the same time of day.
Collection of urine samples for biological monitoring usually is performed using �spot� (i.e., single-void) urine. Logistics and sample integrity become problems when efforts are made to collect urine over extended periods (e.g., 24 hrs). Unless single-void urines are used, numerous opportunities exist for measurement error because of poor control over sample collection, storage and environmental contamination.
To minimize the interval that sample urine resides in the bladder, the following adaption to the �spot� collection procedure is recommended: The bladder should be emptied and then a large glass of water should be consumed; the sample then should be collected within an hour after the water is consumed.
5.3.5 Best Achievable Performance
The best achievable performance is assumed to be equivalent to the performance reported by the manufacturers of the Pharmacia Delphia test kits (Pharmacia 1990). According to the insert that comes with these kits, QC results should be within �2 SDs of the mean for each control sample tested; a CV of less than or equal to 5.2% should be maintained. The total CV reported for test kits is less than or equal to 7.2%.
5.3.6 General Method Performance
Unlike analyses for CDB and CDU, the Pharmacia Delphia test is standardized in a commercial kit that controls for many sources of variation. In the absence of data to the contrary, it is assumed that the achievable performance reported by the manufacturer of this test kit will serve as an achievable performance objective. The CTQ proficiency testing program for B2MU analysis is expected to use the performance parameters defined by the test kit manufacturer as the basis of the B2MU proficiency testing program.
Note that results reported for the test kit are expressed in terms of ?g B2M/l of urine, and have not been adjusted for creatinine. The indicated performance, therefore, is a measure of the performance of the B2M portion of the analyses only, and does not include variation that may have been introduced during the analysis of creatinine.
5.3.7 Observed B2MU Concentrations
As indicated in Section 4.3, the concentration of B2MU may serve as an early indicator of the onset of kidney damage associated with cadmium exposure.
5.3.7.1 Range of B2MU Concentrations Among Unexposed Samples
Most of the studies listed in Table 9 report B2MU levels for those who were not occupationally exposed to cadmium. Studies noted in the second column of this table (which contain the footnote �d�) reported B2MU concentrations among cadmium-exposed workers who, nonetheless, showed no signs of proteinuria. These latter studies are included in this table because, as indicated in Section 4.3, monitoring B2MU is intended to provide advanced warning of the onset of kidney dysfunction associated with cadmium exposure, rather than to distinguish relative exposure. This table, therefore, indicates the range of B2MU levels observed among those who had no symptoms of renal dysfunction (including cadmium-exposed workers with none of these symptoms).
| Study No. | No. in study | Geometric mean | Geometric standard deviation | Lower 95th percentile of distribution a | Upper 95th percentile of distribution a | Reference |
|---|---|---|---|---|---|---|
| 1 | 133 m b | 115 ? g/g c | 4.03 | 12 | 1,140 ?g/g c | Ishizaki et al. 1989. |
| 2 | 161 f b | 146 ?g/g c | 3.11 | 23 | 940 ?g/g c | Ishizaki et al. 1989. |
| 3 | 10 | 84 ?g/g | Ellis et al. 1983. | |||
| 4 | 203 | 76 ?g/l | Stewart and Hughes 1981. | |||
| 5 | 9 | 103 ?g/g | Chia et al. 1989. | |||
| 6 | 47 d | 86 ?g/L | 1.9 | 30 ?g/l | 250 ?g/L | Kjellstrom et al. 1977. |
| 7 | 1,000 e | 68.1 ?g/gr Cr f | 3.1 m & f | <10?g/gr Cr h | 320 ?g/gr Cr h | Kowal 1983. |
| 8 | 87 | 71 ?g/g i | 7 h | 200 h | Buchet et al. 1980. | |
| 9 | 10 | 0.073 mg/24h | Evrin et al. 1971. | |||
| 10 | 59 | 156 ?g/g | 1.1 j | 130 | 180 | Mason et al. 1988. |
| 11 | 8 | 118 ?g/g | Iwao et al. 1980. | |||
| 12 | 34 | 79 ?g/g | Wibowo et al. 1982. | |||
| 13 | 41 m | 400 ?g/gr Cr k | Falck et al. 1983. | |||
| 14 | 35 n | 67 | Roels et al. 1991. | |||
| 15 | 31 d | 63 | Roels et al. 1991. | |||
| 16 | 36 d | 77 i | Miksche et al. 1981. | |||
| 17 | 18 n | 130 | Kawada et al. 1989. | |||
| 18 | 32 p | 122 | Kawada et al. 1989. | |||
| 19 | 18 d | 295 | 1.4 | 170 | 510 | Thun et al. 1989 |
| a Based on an assumed lognormal distribution | ||||||
| b m = males, f = females | ||||||
| c Aged general population from nonpolluted area; 47.9% population aged 50�69; 52.1% ? 70 years of age; values reported in study | ||||||
| d Exposed workers without proteinuria | ||||||
| e 492 females, 484 males | ||||||
| f Creatinine-adjusted; males = 68.1 ?g/g Cr, females = 64.3 ?g/g Cr | ||||||
| h Reported in the study | ||||||
| i Arithmetic mean j Geometric standard error | ||||||
| k Upper 95% tolerance limits: for Falck this is based on the 24 hour urine sample | ||||||
| n Controls | ||||||
| p Exposed synthetic resin and pigment workers without proteinuria; Cadmium in urine levels up to 10 ?g/g Cr | ||||||
To the extent possible, the studies listed in Table 9 provide geometric means and geometric standard deviations for measurements among the groups defined in each study. For studies reporting a geometric standard deviation along with a mean, the lower and upper 95th percentile for these distributions were derived and reported in the table.
The data provided from 15 of the 19 studies listed in Table 9 indicate that the geometric mean concentration of B2M observed among those who were not occupationally exposed to cadmium is 70-170 ?g/g CRTU. Data from the 4 remaining studies indicate that exposed workers who exhibit no signs of proteinuria show mean B2MU levels of 60-300 ?g/g CRTU. B2MU values in the study by Thun et al. (1989), however, appear high in comparison to the other 3 studies. If this study is removed, B2MU levels for those who are not occupationally exposed to cadmium are similar to B2MU levels found among cadmium-exposed workers who exhibit no signs of kidney dysfunction. Although the mean is high in the study by Thun et al., the range of measurements reported in this study is within the ranges reported for the other studies.
Determining a reasonable upper limit from the range of B2M concentrations observed among those who do not exhibit signs of proteinuria is problematic. Elevated B2MU levels are among the signs used to define the onset of kidney dysfunction. Without access to the raw data from the studies listed in Table 9, it is necessary to rely on reported standard deviations to estimate an upper limit for normal B2MU concentrations (i.e., the upper 95th percentile for the distributions measured). For the 8 studies reporting a geometric standard deviation, the upper 95th percentiles for the distributions are 180-1140 ?g/g CRTU. These values are in general agreement with the upper 95th percentile for the distribution (i.e., 631 ?g/g CRTU) reported by Buchet et al. (1980). These upper limits also appear to be in general agreement with B2MU values (i.e., 100-690 ?g/g CRTU) reported as the normal upper limit by Iwao et al. (1980), Kawada et al. (1989), Wibowo et al. (1982), and Schardun and van Epps (1987). These values must be compared to levels reported among those exhibiting kidney dysfunction to define a threshold level for kidney dysfunction related to cadmium exposure.
5.3.7.2 Range of B2MU Concentrations Among Exposed Workers
Table 10 presents results from studies reporting B2MU determinations among those occupationally exposed to cadmium in the work place; in some of these studies, kidney dysfunction was observed among exposed workers, while other studies did not make an effort to distinguish among exposed workers based on kidney dysfunction. As with Table 9, this table provides geometric means and geometric standard deviations for the groups defined in each study if available. For studies reporting a geometric standard deviation along with a mean, the lower and upper 95th percentiles for the distributions are derived and reported in the table.
| Study number | N | Concentration of B-2-microglobulin in urine | Reference | |||
|---|---|---|---|---|---|---|
| Geometric mean (?g/g) a | Geom. Std. Dev. | L 95% of range b | U 95% of range b | |||
| 1 | 1,424 | 160 | 6.19 | 8.1 | 3,300 | Ishizaki et al. 1989. |
| 2 | 1,754 | 260 | 6.50 | 12 | 5,600 | Ishizaki et al. 1989. |
| 3 | 33 | 210 | Ellis et al. 1983. | |||
| 4 | 65 | 210 | Chia et al. 1989. | |||
| 5 | c 44 | 5,700 | 6.49 | d 300 | d 98,000 | Kjellstrom et al. 1977. |
| 6 | 148 | e 180 | f 110 | f280 | Buchet et al. 1980. | |
| 7 | 37 | 160 | 3.90 | 17 | 1,500 | Kenzaburo et al. 1979. |
| 8 | c 45 | 3,300 | 8.70 | d 310 | d 89,000 | Mason et al. 1988. |
| 9 | c 10 | 6,100 | 5.99 | f 650 | f 57,000 | Falck et al. 1983. |
| 10 | c 11 | 3,900 | 2.96 | d 710 | d 15,000 | Elinder et al. 1985. |
| 11 | c 12 | 300 | Roels et al. 1991. | |||
| 12 | g 8 | 7,400 | Roels et al. 1991. | |||
| 13 | c 23 | h 1,800 | Roels et al. 1989. | |||
| 14 | 10 | 690 | Iwao et al. 1980. | |||
| 15 | 34 | 71 | Wibowo et al. 1982. | |||
| 16 | c 15 | 4,700 | 6.49 | d 590 | d 93,000 | Thun et al. 1989. |
| a Unless otherwise stated. | ||||||
| b Based on an assumed lognormal distribution. | ||||||
| c Among workers diagnosed as having renal dysfunction; for Elinder this means ? 2 levels greater than 300 micrograms per gram creatinine (?g/gr Cr); for Roels, 1991, range=31�35, 170 ?g? 2 /gr Cr and geometric mean=63 among healthy workers; for Mason ? 2 300 ?g/gr Cr. | ||||||
| d Based on a detailed review of the data by OSHA. | ||||||
| e Arithmetic mean. | ||||||
| f Reported in the study. | ||||||
| g Retired workers. | ||||||
| h 1,800 ?g? 2 /gr Cr for first survey; second survey=1,600; third survey=2,600; fourth survey=2,600; fifth survey=2,600. | ||||||
The data provided in Table 10 indicate that the mean B2MU concentration observed among workers experiencing occupational exposure to cadmium (but with undefined levels of proteinuria) is 160�7400 ?g/g CRTU. One of these studies reports geometric means lower than this range (i.e., as low as 71 ?g/g CRTU); an explanation for this wide spread in average concentrations is not available.
Seven of the studies listed in Table 10 report a range of B2MU levels among those diagnosed as having renal dysfunction. As indicated in this table, renal dysfunction (proteinuria) is defined in several of these studies by B2MU levels in excess of 300 ?g/g CRTU (see footnote �c� of Table 10); therefore, the range of B2MU levels observed in these studies is a function of the operational definition used to identify those with renal dysfunction. Nevertheless, a B2MU level of 300 ?g/g CRTU appears to be a meaningful threshold for identifying those having early signs of kidney damage. While levels much higher than 300 ?g/g CRTU have been observed among those with renal dysfunction, the vast majority of those not occupationally exposed to cadmium exhibit much lower B2MU concentrations (see Table 9). Similarly, the vast majority of workers not exhibiting renal dysfunction are found to have levels below 300 ?g/g CRTU (Table 9).
The 300 ?g/g CRTU level for B2MU proposed in the above Paragraph has support among researchers as the threshold level that distinguishes between cadmium-exposed workers with and without kidney dysfunction. For example, in the guide for physicians who must evaluate cadmium-exposed workers written for the Cadmium Council by Dr. Lauwerys, levels of B2M greater than 200-300 ?g/g CRTU are considered to require additional medical evaluation for kidney dysfunction (exhibit 8-447, OSHA docket H057A). The most widely used test for measuring B2M (i.e., the Pharmacia Delphia test) defines B2MU levels above 300 ?g/l as abnormal (exhibit L-140-1, OSHA docket H057A).
Dr. Elinder, chairman of the Department of Nephrology at the Karolinska Institute, testified at the hearings on the proposed cadmium rule. According to Dr. Elinder (exhibit L-140-45, OSHA docket H057A), the normal concentration of B2MU has been well documented (Evrin and Wibell 1972; Kjellstrom et al. 1977a; Elinder et al. 1978, 1983; Buchet et al. 1980; Jawaid et al. 1983; Kowal and Zirkes, 1983). Elinder stated that the upper 95 or 97.5 percentiles for B2MU among those without tubular dysfunction is below 300 ?g/g CRTU (Kjellstrom et al. 1977a; Buchet et al. 1980; Kowal and Zirkes, 1983). Elinder defined levels of B2M above 300 ?g/g CRTU as �slight� proteinuria.
5.3.8 Conclusions and Recommendations for B2MU
Based on the above evaluation, the following recommendations are made for a B2MU proficiency testing program. Note that the following discussion addresses only sampling and analysis for B2MU determinations (i.e., to be reported as an unadjusted ?g B2M/l urine). Normalizing this result to creatinine requires a second analysis for CRTU (see section 5.4) so that the ratio of the 2 measurements can be obtained.
5.3.8.1 Recommended Method
The Pharmacia Delphia method (Pharmacia 1990) should be adopted as the standard method for B2MU determinations. Laboratories may adopt alternate methods, but it is the responsibility of the laboratory to demonstrate that alternate methods provide results of comparable quality to the Pharmacia Delphia method.
5.3.8.2 Data Quality Objectives
The following data quality objectives should facilitate interpretation of analytical results, and should be achievable based on the above evaluation.
Limit of Detection. A limit of 100 ?g/l urine should be achievable, although the insert to the test kit (Pharmacia 1990) cites a detection limit of 150 ?g/l; private conversations with representatives of Pharmacia, how ever, indicate that the lower limit of 100 ?g/l should be achievable provided an additional standard of 100 ?g/l B2M is run with the other standards to derive the calibration curve (section 3.3.1.1). The lower detection limit is desirable due to the proximity of this detection limit to B2MU values defined for the cadmium medical monitoring program.
Accuracy. Because results from an interlaboratory proficiency testing program are not available currently, it is difficult to define an achievable level of accuracy. Given the general performance parameters defined by the insert to the test kits, however, an accuracy of � 15% of the target value appears achievable.
Due to the low levels of B2MU to be measured generally, it is anticipated that the analysis of creatinine will contribute relatively little to the overall variability observed among creatinine-normalized B2MU levels (see section 5.4). The initial level of accuracy for reporting B2MU levels under this program should be set at � 15%.
Precision. Based on precision data reported by Pharmacia (1990), a precision value (i.e., CV) of 5% should be achievable over the defined range of the analyte. For internal QC samples (i.e., recommended as part of an internal QA/QC program, section 3.3.1), laboratories should attain precision near 5% over the range of concentrations measured.
5.3.8.3 Quality Assurance/Quality Control
Commercial laboratories providing measurement of B2MU should adopt an internal QA/QC program that incorporates the following components: Strict adherence to the Pharmacia Delphia method, including calibration requirements; regular use of QC samples during routine runs; a protocol for corrective actions, and documentation of these actions; and, participation in an interlaboratory proficiency program. Procedures that may be used to address internal QC requirements are presented in Attachment 1. Due to differences between analyses for B2MU and CDB/CDU, specific values presented in Attachment 1 may have to be modified. Other components of the program (including characterization runs), however, can be adapted to a program for B2MU.
5.4 Monitoring Creatinine in Urine (CRTU)
Because CDU and B2MU should be reported relative to concentrations of CRTU, these concentrations should be determined in addition CDU and B2MU determinations.
5.4.1 Units of CRTU Measurement
CDU should be reported as ?g Cd/g CRTU, while B2MU should be reported as ?g B2M/g CRTU. To derive the ratio of cadmium or B2M to creatinine, CRTU should be reported in units of g crtn/l of urine. Depending on the analytical method, it may be necessary to convert results of creatinine determinations accordingly.
5.4.2 Analytical Techniques Used To Monitor CRTU
Of the techniques available for CRTU determinations, an absorbance spectrophotometric technique and a high-performance liquid chromatography (HPLC) technique are identified as acceptable in this protocol.
5.4.3 Methods Developed for CRTU Determinations
CRTU analysis performed in support of either CDU or B2MU determinations should be performed using either of the following 2 methods:
1. The Du Pont method (i.e., Jaffe method), in which creatinine in a sample reacts with picrate under alkaline conditions, and the resulting red chromophore is monitored (at 510 nm) for a fixed interval to determine the rate of the reaction; this reaction rate is proportional to the concentration of creatinine present in the sample (a copy of this method is provided in Attachment 2 of this protocol); or
2. The OSHA SLC Technical Center (OSLTC) method, in which creatinine in an aliquot of sample is separated using an HPLC column equipped with a UV detector; the resulting peak is quantified using an electrical integrator (a copy of this method is provided in Attachment 3 of this protocol).
5.4.4 Sample Collection and Handling
CRTU samples should be segregated from samples collected for CDU or B2MU analysis. Sample-collection techniques have been described under section 5.2.4. Samples should be preserved either to stabilize CDU (with HNO 3 ) or B2MU (with NaOH). Neither of these procedures should adversely affect CRTU analysis (see Attachment 3).
5.4.5 General Method Performance
Data from the OSLTC indicate that a CV of 5% should be achievable using the OSLTC method (Septon, L private communication). The achievable accuracy of this method has not been determined.
Results reported in surveys conducted by the CAP (CAP 1991a, 1991b and 1992) indicate that a CV of 5% is achievable. The accuracy achievable for CRTU determinations has not been reported.
Laboratories performing creatinine analysis under this protocol should be CAP accredited and should be active participants in the CAP surveys.
5.4.6 Observed CRTU Concentrations
Published data suggest the range of CRTU concentrations is 1.0-1.6 ?g in 24-hour urine samples (Harrison 1987). These values are equivalent to about 1 ?g/l urine.
5.4.7 Conclusions and Recommendations for CRTU
5.4.7.1 Recommended Method
Use either the Jaffe method (Attachment 2) or the OSLTC method (Attachment 3). Alternate methods may be acceptable provided adequate performance is demonstrated in the CAP program.
5.4.7.2 Data Quality Objectives
Limit of Detection. This value has not been formally defined; however, a value of 0.1 ?g/l urine should be readily achievable.
Accuracy. This value has not been defined formally; accuracy should be sufficient to retain accreditation from the CAP.
Precision. A CV of 5% should be achievable using the recommended methods.
6.0 References
Adamsson E, Piscator M, and Nogawa K. (1979). Pulmonary and gastrointestinal exposure to cadmium oxide dust in a battery factory. Environmental Health Perspectives, 28, 219-222.
American Conference of Governmental Industrial Hygienists (ACGIH). (1986). Documentation of the Threshold Limit Values and Biological Exposure Indices. 5th edition. p. BEI-55.
Bernard A, Buchet J, Roels H, Masson P, and Lauwerys R. (1979). Renal excretion of proteins and enzymes in workers exposed to cadmium. European Journal of Clinical Investigation, 9, 11-22.
Bernard A and Lauwerys R. (1990). Early markers of cadmium neph-rotoxicity: Biological significance and predictive value. Toxocological and Environmental Chemistry, 27, 65-72.
Braunwald E, Isselbacher K, Petersdorf R, Wilson J, Martin J, and Fauci A (Eds.). (1987). Harrison�s Principles of Internal Medicine. New York: McGraw-Hill Book Company.
Buchet J, Roels H, Bernard I, and Lauwerys R. (1980). Assessment of renal funcion of workers exposed to inorganic lead, cadmium, or mercury vapor. Journal of Occupational Medicine, 22, 741-750.
CAP. (1991). Urine Chemistry, Series 1: Survey (Set U-B). College of American Pathologists.
CAP. (1991). Urine Chemistry, Series 1: Survey (Set U-C). College of American Pathologists.
CAP. (1992). Urine Chemistry, Series 1: Survey (Set U-A). College of American Pathologists.
CDC. (1986). Centers for Disease Control, Division of Environmental Health Laboratory Sciences, Center for Environmental Health, Atlanta, Georgia. Docket No. 106A. Lake Couer d�Alene, Idaho cadmium and lead study: 86-0030, Specimen collection and shipping protocol.
CDC. (1990). Centers for Disease Control, Nutritional Biochemistry Branch. 4/27/90 Draft SOP for Method 0360A �Determination of cadmium in urine by graphite furnace atomic absorption spectrometry with Zeeman background correction.�
Centre de Toxicologie du Quebec. (1991). Interlaboratory comparison program report for run 2. Shipping date 3/11/91. Addition BLR 9/19.
Chia K, Ong C, Ong H, and Endo G. (1989). Renal tubular function of workers exposed to low levels of cadmium. British Journal of Industrial Medicine, 46, 165-170.
Claeys-Thoreau F. (1982). Determination of low levels of cadmium and lead in biological fluids with simple dilution by atomic absorption spectrophotometry using Zeeman effect background absorption and the L�Vov platform. Atomic Spectroscopy, 3, 188-191.
DeBenzo Z, Fraile R, and Carrion N. (1990). Electrothermal atomization atomic absorption spectrometry with stabilized aqueous standards for the determination of cadmium in whole blood. Analytica Chimica Acta, 231, 283-288.
Elinder C, Edling C, Lindberg E, Kagedal B, and Vesterberg O. (1985). Assessment of renal function in workers previously exposed to cadmium. British Journal of Internal Medicine, 42,754.
Ellis K, Cohn S, and Smith T. (1985). Cadmium inhalation exposure estimates: Their significance with respect to kidney and liver cadmium burden. Journal of Toxicology and Environmental Health, 15, 173-187.
Ellis K, Yasumura S, Vartsky D, and Cohn S. (1983). Evaluation of biological indicators of body burden of cadmium in humans. Fundamentals and Applied Toxicology, 3, 169-174.
Ellis K, Yeun K, Yasumura S, and Cohn S. (1984). Dose-response analysis of cadmium in man: Body burden vs kidney function. Environmental Research, 33, 216-226.
Evrin P, Peterson A, Wide I, and Berggard I. (1971). Radioimmunoassay of B-2-microglobulin in human biological fluids. Scandanavian Journal of Clinical Laboratory Investigation, 28, 439-443.
Falck F, Fine L, Smith R, Garvey J, Schork A, England B, McClatchey K, and Linton J. (1983). Metallothionein and occupational exposure to cadmium. British Journal of Industrial Medicine, 40, 305-313.
Federal Register. (1990). Occupational exposure to cadmium: Proposed rule. 55/22/4052-4147, February 6.
Friberg, Exhibit 29, (1990). Exhibit No. 29 of the OSHA Federal Docket H057A. Washington, D.C.
Friberg L. (1988). Quality assurance. In T. Clarkson (Ed.), Biological Monitoring of Toxic Metals (pp. 103-105). New York: Plenum Press.
Friberg L. and Elinder C. (1988). Cadmium toxicity in humans. In Essential and Trace Elements in Human Health and Disease (pp. 559-587). Docket Number 8-660.
Friberg L., Elinder F., et al. (1986). Cadmium and Health: A Toxicological and Epidemiological Appraisal. Volume II, Effects and Response. Boca Raton, FL: CRC Press.
Friberg L., Piscator M., Nordberg G., and Kjellstrom T. (1974). Cadmium in the Environment (2nd ed.). Cleveland: CRC.
Friberg L., and Vahter M. (1983). Assessment of exposure to lead and cadmium through biological monitoring: Results of a UNEP/WHO global study. Environmental Research, 30, 95-128.
Gunter E., and Miller D. (1986). Laboratory procedures used by the division of environmental health laboratory sciences center for environmental health, Centers for Disease Control for the Hispanic health and nutrition examination survey (HHANES). Atlanta, GA: Centers for Disease Control.
Harrison. (1987). Harrison�s Principles of Internal Medicine. Braun-wald, E; Isselbacher, KJ; Petersdorf, RG; Wilson, JD; Martin, JB; and Fauci, AS Eds. Eleventh Ed. McGraw Hill Book Company. San Francisco.
Henry J. (1991). Clinical Diagnosis and Management by Laboratory Methods (18th edition). Philadelphia: WB Saunders Company.
IARC. (1987). IRAC Monographs on the Evaluation of Carcinogenic Risks to Humans. Overall Evaluation of Carcinogenicity: Update of Volume 1-42. Supplemental 7, 1987.
Ishizaki M., Kido T., Honda R., Tsuritani I., Yamada Y., Nakagawa H., and Nogawa K. (1989). Dose-response relationship between urinary cadmium and B-2-microglobulin in a Japanese environmentally cadmium exposed population. Toxicology, 58, 121-131.
Iwao S., Tsuchiya K., and Sakurai H. (1980). Serum and urinary B-2-microglobulin among cadmium-exposed workers. Journal of Occupational Medicine, 22, 399-402.
Iwata K., Katoh T., Morikawa Y., Aoshima K., Nishijo M., Teranishi H., and Kasuya M. (1988). Urinary trehalase activity as an indicator of kidney injury due to environmental cadmium exposure. Archives of Toxicology, 62, 435-439.
Kawada T., Koyama H., and Suzuki S. (1989). Cadmium, NAG activity, and B-2-microglobulin in the urine of cadmium pigment workers. British Journal of Industrial Medicine, 46, 52-55.
Kawada T., Tohyama C., and Suzuki S. (1990). Significance of the excretion of urinary indicator proteins for a low level of occupational exposure to cadmium. International Archives of Occupational Environmental Health, 62, 95-100.
Kjellstrom T. (1979). Exposure and accumulation of cadmium in populations from Japan, the United States, and Sweden. Environmental Health Perspectives, 28, 169-197.
Kjellstrom T., Evrin P., and Rahnster B. (1977). Dose-response analysis of cadmium-induced tubular proteinuria. Environmental Research, 13, 303-317.
Kjellstrom T., Shiroishi K., and Evrin P. (1977). Urinary B-2-microglobulin excretion among people exposed to cadmium in the general environment. Environmental Research, 13, 318-344.
Kneip T., & Crable J. (Eds.). (1988). Method 107. Cadmium in blood. Methods for biological monitoring (pp.161�164). Washington, DC: American Public Health Association.
Kowal N. (1988). Urinary cadmium and B-2-microglobulin: Correlation with nutrition and smoking history. Journal of Toxicology and Environmental Health, 25, 179-183.
Kowal N., Johnson D., Kraemer D., and Pahren H. (1979). Normal levels of cadmium in diet, urine, blood, and tissues of inhabitants of the United States. Journal of Toxicology and Environmental Health, 5, 995-1014.
Kowal N. and Zirkes M. (1983). Urinary cadmium and B-2-microglobulin: Normal values and concentration adjustment. Journal of Toxicology and Environmental Health, 11, 607-624.
Lauwerys R., Buchet J., and Roels H. (1976). The relationship between cadmium exposure or body burden and the concentration of cadmium in blood and urine in man. International Archives of Occupational and Environmental Health, 36, 275-285.
Lauwerys R, Roels H, Regniers, Buchet J, and Bernard A. (1979). Significance of cadmium concentration in blood and in urine in workers exposed to cadmium. Environmental Research, 20, 375-391.
Lind B, Elinder C, Friberg L, Nilsson B, Svartengren M, and Vahter M. (1987). Quality control in the analysis of lead and cadmium in blood. Fre-senius� Zeitschrift fur Analytical Chemistry, 326, 647-655.
Mason H, Davison A, Wright A, Guthrie C, Fayers P, Venables K, Smith N, Chettle D, Franklin D, Scott M, Holden H, Gompertz D, and Newman-Taylor A. (1988). Relations between liver cadmium, cumulative exposure, and renal function in cadmium alloy workers. British Journal of Industrial Medicine, 45, 793-802.
Meridian Research, Inc. (1989). Quantitative Assessment of Cancer Risks Associated with Occupational Exposure to Cd. Prepared by Meridian Research, Inc. and Roth Associates, Inc. for the Occupational Safety & Health Administration. June 12,1989.
Meridian Research, Inc and Roth Associates, Inc. (1989). Quantitative Assessment of the Risk of Kidney Dysfunction Associated with Occupational Exposure to Cd. Prepared by Meridian Research, Inc. and Roth Associates, Inc. for the Occupational Safety & Health Administration. July 31 1989.
Micheils E and DeBievre P. (1986). Method 25�Determination of cadmium in whole blood by isotope dilution mass spectrometry. O�Neill I, Schuller P, and Fishbein L (Eds.), Environmental Carcinogens Selected Methods of Analysis (Vol. 8). Lyon, France: International Agency for Research on Cancer.
Mueller P, Smith S, Steinberg K, and Thun M. (1989). Chronic renal tubular effects in relation to urine cadmium levels. Nephron, 52, 45-54.
NIOSH. (1984a). Elements in blood or tissues. Method 8005 issued 5/15/85 and Metals in urine. Method 8310 issued 2/15/84 In P. Eller (Ed.), NIOSH Manual of Analytical Methods (Vol.1, Ed. 3). Cincinnati, Ohio: US-DHHS.
NIOSH. (1984b). Lowry L. Section F: Special considerations for biological samples in NIOSH Manual of Analytical Methods (Vol. 1, 3rd ed). P. Eller (Ed.). Cincinnati, Ohio: US-DHHS.
Nordberg G and Nordberg M. (1988). Biological monitoring of cadmium. In T. Clarkson, L. Friberg, G. Nordberg, and P. Sager (Eds.), Biological Monitoring of Toxic Metals, New York: Plenum Press.
Nogawa K. (1984). Biologic indicators of cadmium nephrotoxicity in persons with low-level cadmium exposure. Environmental Health Perspectives, 54, 163-169.
OSLTC (no date). Analysis of Creatinine for the Normalization of Cadmium and Beta-2-Microglobulin Concentrations in Urine. OSHA Salt Lake Technical Center. Salt Lake City, UT.
Paschal. (1990). Attachment 8 of exhibit 106 of the OSHA docket H057A.
Perkin-Elmer Corporation. (1982). Analytical Methods for Atomic Absorption Spectroscopy.
Perkin-Elmer Corporation. (1977). Analytical Methods Using the HGA Graphite Furnace.
Pharmacia Diagnostics. (1990). Pharmacia DELFIA system B-2-microglobulin kit insert. Uppsala, Sweden: Pharmacia Diagnostics.
Piscator M. (1962). Proteinuria in chronic cadmium poisoning. Archives of Environmental Health, 5, 55-62.
Potts, C.L. (1965). Cadmium Proteinuria�The Health Battery Workers Exposed to Cadmium Oxide dust. Ann Occup Hyg, 3:55-61, 1965.
Princi F. (1947). A study of industrial exposures to cadmium. Journal of Industrial Hygiene and Toxicology, 29, 315-320.
Pruszkowska E, Carnick G, and Slavin W. (1983). Direct determination of cadmium in urine with use of a stabilized temperature platform furnace and Zeeman background correction. Clinical Chemistry, 29, 477-480.
Roberts C and Clark J. (1986). Improved determination of cadmium in blood and plasma by flameless atomic absorption spectroscopy. Bulletin of Environmental Contamination and Toxicology, 36, 496-499.
Roelandts I. (1989). Biological reference materials. Soectrochimica Acta, 44B, 281-290.
Roels H, Buchet R, Lauwerys R, Bruaux P, Clays-Thoreau F, Laafon-taine A, Overschelde J, and Verduyn J. (1978). Lead and cadmium absorption among children near a nonferrous metal plant. Environmental Research, 15, 290-308.
Roels H, Djubgang J, Buchet J, Bernard A, and Lauwerys R. (1982). Evolution of cadmium-induced renal dysfunction in workers removed from exposure. Scandanavian Journal of Work and Environmental Health, 8, 191-200.
Roels H, Lauwerys R, and Buchet J. (1989). Health significance of cadmium induced renal dysfunction: A five year follow-up. British Journal of Industrial Medicine, 46, 755-764.
Roels J, Lauwerys R, Buchet J, Bernard A, Chettle D, Harvey T, and Al-Haddad I. (1981). In vivo measurements of liver and kidney cadmium in workers exposed to this metal: Its significance with respect to cadmium in blood and urine. Environmental Research, 26, 217-240.
Roels H, Lauwerys R, Buchet J, Bernard A, Lijnen P, and Houte G. (1990). Urinary kallikrein activity in workers exposed to cadmium, lead, or mercury vapor. British Journal of Industrial Medicine, 47, 331-337.
Sakurai H, Omae K, Toyama T, Higashi T, and Nakadate T. (1982). Cross-sectional study of pulmonary function in cadmium alloy workers. Scandanavian Journal of Work and Environmental Health, 8, 122-130.
Schardun G and van Epps L. (1987). B-2-microglobulin: Its significance in the evaluation of renal function. Kidney International, 32, 635-641.
Shaikh Z, and Smith L. (1984). Biological indicators of cadmium exposure and toxicity. Experentia, 40, 36-43.
Smith J and Kench J. (1957). Observations on urinary cadmium and protein excretion in men exposed to cadmium oxide dust and fume. Brit-ish Journal of Industrial Medicine, 14, 240-245.
Smith J, Kench J, and Lane R. (1955). Determination of Cadmium in urine and observations on urinary cadmium and protein excretion in men exposed to cadmium oxide dust. British Journal of Industrial Medicine, 12, 698-701.
SWRI (Southwest Research Institute). (1978). The distribution of cadmium and other metals in human tissues. Health Effects Research Lab, Research Triangle Park, NC, Population Studies Division. NTIS No. PB-285-200.
Stewart M and Hughes E. (1981). Urinary B-2-microglobulin in the biological monitoring of cadmium workers. British Journal of Industrial Medicine, 38, 170-174.
Stoeppler K and Brandt M. (1980). Contributions to automated trace analysis. Part V. Determination of cadmium in whole blood and urine by electrothermal atomic absorption spectrophotometry. Fresenius� Zeitsch-rift fur Analytical Chemistry, 300, 372-380.
Takenaka et al. (1983). Carcinogencity of Cd Chloride Aerosols in White Rats. INCI 70: 367-373, 1983.
Thun M, Osorio A, Schober S, Hannon W, Lewis B, and Halperin W. (1989). Nephropathy in cadmium workers: Assessment of risk from airborne occupational exposure to cadmium. British Journal of Industrial Medicine, 46, 689-697.
Thun M, Schnorr T, Smith A, Halperin W, and Lemen R. (1985). Mortality among a cohort of US cadmium production workers--an update. Journal of the National Cancer Institute, 74,325-333.
Travis D and Haddock A. (1980). Interpretation of the observed age-dependency of cadmium body burdens in man. Environmental Research, 22, 46-60.
Tsuchiya K. (1967). Proteinuria of workers exposed to cadmium fume. Archives of Environmental Health, 14, 875-880.
Tsuchiya K. (1976). Proteinuria of cadmium workers. Journal of Occupational Medicine, 18, 463-470.
Tsuchiya K, Iwao S, Sugita M, Sakurai H. (1979). Increased urinary B-2-microglobulin in cadmium exposure: Dose-effect relationship and biological significance of B-2-microglobulin. Environmental Health Perspectives, 28, 147-153.
USEPA. (1985). Updated Mutagenicity and Carcinogenicity Assessments of Cd: Addendum to the Health Assessment Document for Cd (May 1981). Final Report. June 1985.
Vahter M and Friberg L. (1988). Quality control in integrated human exposure monitoring of lead and cadmium. Fresenius� Zeitschrift fur Analytical Chemistry, 332, 726-731.
Weber J. (1988). An interlaboratory comparison programme for several toxic substances in blood and urine. The Science of the Total Environment, 71, 111-123.
Weber J. (1991a). Accuracy and precision of trace metal determinations in biological fluids. In K. Subramanian, G. Iyengar, and K. Okamot (Eds.), Biological Trace Element Research-Multidisciplinary Perspectives, ACS Symposium Series 445. Washington, DC: American Chemical Society.
Weber J. (1991b). Personal communication about interlaboratory program and shipping biological media samples for cadmium analyses.
Wibowo A, Herber R, van Deyck W, and Zielhuis R. (1982). Biological assessment of exposure in factories with second degree usage of cadmium compounds. International Archives of Occupational Environmental Health, 49, 265-273.
Attachment 1�Nonmandatory Protocol for an Internal Quality Assurance/Quality Control Program
The following is an example of the type of internal quality assurance/quality control program that assures adequate control to satisfy OSHA requirements under this protocol. However, other approaches may also be acceptable.
As indicated in Section 3.3.1 of the protocol, the QA/QC program for CDB and CDU should address, at a minimum, the following:
- Calibration;
- Establishment of control limits;
- Internal QC analyses and maintaining control; and
- Corrective action protocols.
This illustrative program includes both initial characterization runs to establish the performance of the method and ongoing analysis of quality control samples intermixed with compliance samples to maintain control.
Calibration
Before any analytical runs are conducted, the analytic instrument must be calibrated. This is to be done at the beginning of each day on which quality control samples and/or compliance samples are run. Once calibration is established, quality control samples or compliance samples may be run. Regardless of the type of samples run, every fifth sample must be a standard to assure that the calibration is holding.
Calibration is defined as holding if every standard is within plus or minus (�) 15% of its theoretical value. If a standard is more than plus or minus 15% of its theoretical value, then the run is out of control due to calibration error and the entire set of samples must either be reanalyzed after recalibrating or results should be recalculated based on a statistical curve derived from the measurement of all standards.
It is essential that the highest standard run is higher than the highest sample run. To assure that this is the case, it may be necessary to run a high standard at the end of the run, which is selected based on the results obtained over the course of the run.
All standards should be kept fresh, and as they get old, they should be compared with new standards and replaced if they exceed the new standard by � 15%.
Initial Characterization Runs and Establishing Control
A participating laboratory should establish four pools of quality control samples for each of the analytes for which determinations will be made. The concentrations of quality control samples within each pool are to be centered around each of the four target levels for the particular analyte identified in Section 4.4 of the protocol.
Within each pool, at least 4 quality control samples need to be established with varying concentrations ranging between plus or minus 50% of the target value of that pool. Thus for the medium-high cadmium in blood pool, the theoretical values of the quality control samples may range from 5 to 15 ?g/l, (the target value is 10 ?g/l). At least 4 unique theoretical values must be represented in this pool.
The range of theoretical values of plus or minus 50% of the target value of a pool means that there will be overlap of the pools. For example, the range of values for the medium-low pool for cadmium in blood is 3.5 to 10.5 ?g/l while the range of values for the medium-high pool is 5 to 15 ?g/l. Therefore, it is possible for a quality control sample from the medium-low pool to have a higher concentration of cadmium than a quality control sample from the medium-high pool.
Quality control samples may be obtained as commercially available reference materials, internally prepared, or both. Internally prepared samples should be well characterized and traced or compared to a reference material for which a consensus value for concentration is available. Levels of analyte in the quality control samples must be concealed from the analyst prior to the reporting of analytical results. Potential sources of materials that may be used to construct quality control samples are listed in Section 3.3.1 of the protocol.
Before any compliance samples are analyzed, control limits must be established. Control limits should be calculated for every pool of each analyte for which determinations will be made, and control charts should be kept for each pool of each analyte. A separate set of control charts and control limits should be established for each analytical instrument in a laboratory that will be used for analysis of compliance samples.
At the beginning of this QA/QC program, control limits should be based on the results of the analysis of 20 quality control samples from each pool of each analyte. For any given pool, the 20 quality control samples should be run on 20 different days. Although no more than one sample should be run from any single pool on a particular day, a laboratory may run quality control samples from different pools on the same day. This constitutes a set of initial characterization runs.
For each quality control sample analyzed, the value F/T (defined in the glossary) should be calculated. To calculate the control limits for a pool of an analyte, it is first necessary to calculate the mean, X?, of the F/T values for each quality control sample in a pool and then to calculate its standard deviation, �. Thus, for the control limit for a pool, X? is calculated as:
 |
and � is calculated as
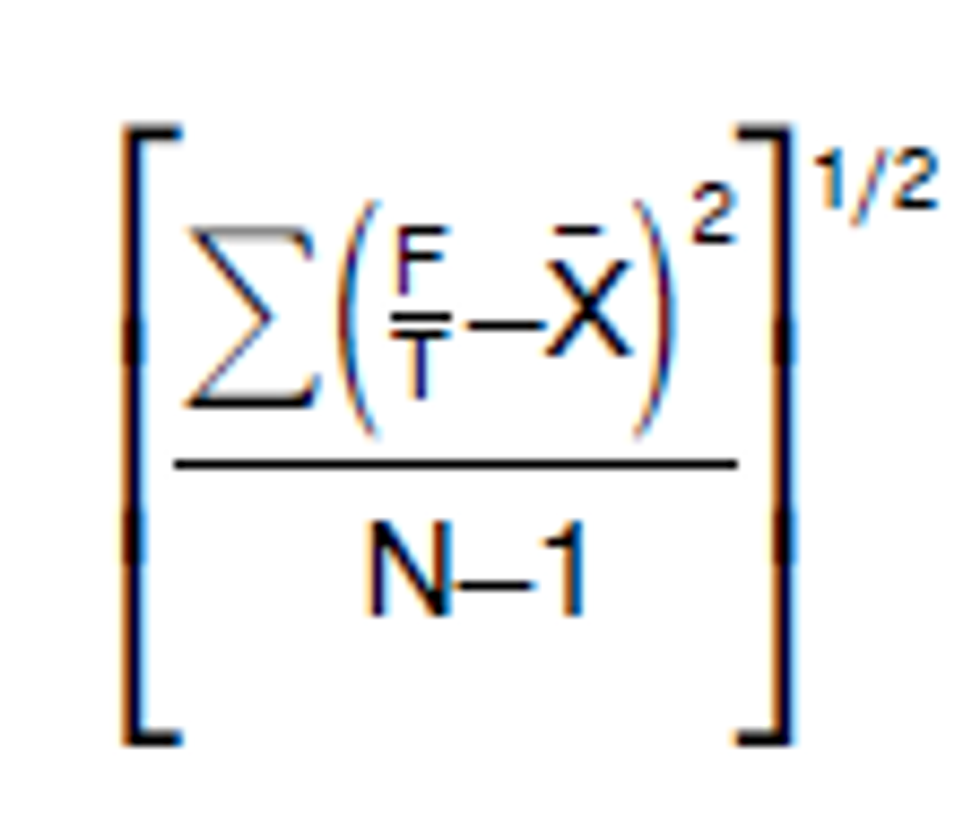 |
| where N is the number of quality control samples run for a pool. |
The control limit for a particular pool is then given by the mean plus or minus 2 standard deviations (X? � 2 � ). The control limits may be no greater than 40% of the mean F/T value. If three standard deviations are greater than 40% of the mean F/T value, then analysis of compliance samples may not begin. 1 Instead, an investigation into the causes of the large standard deviation should begin, and the inadequacies must be remedied. Then, control limits must be reestablished which will mean repeating the running 20 quality control samples from each pool over 20 days.
Internal Quality Control Analyses and Maintaining Control
Once control limits have been established for each pool of an analyte, analysis of compliance samples may begin. During any run of compliance samples, quality control samples are to be interspersed at a rate of no less than 5% of the compliance sample workload. When quality control samples are run, however, they should be run in sets consisting of one quality control sample from each pool. Therefore, it may be necessary, at times, to intersperse quality control samples at a rate greater than 5%.
There should be at least one set of quality control samples run with any analysis of compliance samples. At a minimum, for example, 4 quality control samples should be run even if only 1 compliance sample is run. Generally, the number of quality control samples that should be run are a multiple of four with the minimum equal to the smallest multiple of four that is greater than 5% of the total number of samples to be run. For example, if 300 compliance samples of an analyte are run, then at least 16 quality control samples should be run (16 is the smallest multiple of four that is greater than 15, which is 5% of 300).
Control charts for each pool of an analyte (and for each instrument in the laboratory to be used for analysis of compliance samples) should be established by plotting F/T versus date as the quality control sample results are reported. On the graph there should be lines representing the control limits for the pool, the mean F/T limits for the pool, and the theoretical F/T of 1.000. Lines representing plus or minus (�) 2 � should also be represented on the charts. A theoretical example of a control chart is presented in Figure 1.
Note that the value, �40%� may change over time as experience is gained with the program.
 |
All quality control samples should be plotted on the chart, and the charts should be checked for visual trends. If a quality control sample falls above or below the control limits for its pool, then corrective steps must be taken (see the section on corrective actions below). Once a laboratory�s program has been established, control limits should be updated every 2 months.
The updated control limits should be calculated from the results of the last 100 quality control samples run for each pool. If 100 quality control samples from a pool have not been run at the time of the update, then the limits should be based on as many as have been run provided at least 20 quality control samples from each pool have been run over 20 different days.
The trends that should be looked for on the control charts are:
1. 10 consecutive quality control samples falling above or below the mean;
2. 3 consecutive quality control samples falling more than 2 � from the mean (above or below the 2 � lines of the chart); or
3. the mean calculated to update the control limits falls more than 10% above or below the theoretical mean of 1.000.
If any of these trends is observed, then all analysis must be stopped, and an investigation into the causes of the errors must begin. Before the analysis of compliance samples may resume, the inadequacies must be remedied and the control limits must be reestablished for that pool of an analyte. Reestablishment of control limits will entail running 20 sets of quality control samples over 20 days.
Note that alternative procedures for defining internal quality control limits may also be acceptable. Limits may be based, for example, on proficiency testing, such as � 1?g or 15% of the mean (whichever is greater). These should be clearly defined.
Corrective Actions
Corrective action is the term used to describe the identification and remediation of errors occurring within an analysis. Corrective action is necessary whenever the result of the analysis of any quality control sample falls outside of the established control limits. The steps involved may include simple things like checking calculations of basic instrument maintenance, or it may involve more complicated actions like major instrument repair. Whatever the source of error, it must be identified and corrected (and a Corrective Action Report (CAR) must be completed. CARs should be kept on file by the laboratory.
Attachment 2
Creatinine in Urine (JAFFE PROCEDURE).
Intended Use: The CREA pack is used in the Du Pont ACA� discrete clinical analyzer to quantitatively measure creatinine in serum and urine.
Summary: The CREA method employs a modification of the kinetic Jaffe reaction reported by Larsen. This method has been reported to be less susceptible than conventional methods to interference from non-creatinine, Jaffe-positive compounds.
A split sample comparison between the CREA method and a conventional Jaffe procedure on Autoanalyzer� showed a good correlation. (See Specific Performance Characteristics).
*Note: Numbered subscripts refer to the bibliography and lettered subscripts refer to footnotes.
Autoanalyzer� is a registered trademark of Technicon Corp., Tarrytown, NY.
Principles of Procedure: In the presence of a strong base such as NaOH, picrate reacts with creatinine to form a red chromophore. The rate of increasing absorbance at 510 nm due to the formation of this chromophore during a 17.07-second measurement period is directly proportional to the creatinine concentration in the sample.
 |
| Compartment a | Form | Ingredient | Quantity b |
|---|---|---|---|
| No. 2, 3, & 4.. | Liquid | Picrate | 0.11 mmol. |
| No6 | Liquid | NaOH (for pH adjustment) c | |
| a Compartments are numbered 1-7, with compartment #7 located clos est to pack fill position #2. | |||
| b Nominal value at manufacture. | |||
| c See Precautions. | |||
Precautions: Compartment #6 contains 75?L of 10 N NaOH; avoid contact; skin irritant; rinse contacted area with water. Comply With OSHA�s Bloodborne Pathogens Standard While Handling Biological Samples (29 CFR 1910.1039).
Used packs contain human body fluids; handle with appropriate care.
FOR IN VITRO DIAGNOSTIC USE.
Mixing and Diluting:
Mixing and diluting are automatically performed by the ACA� discrete clinical analyzer. The sample cup must contain sufficient quantity to accommodate the sample volume plus the "dead volume" precise cup filling is not required.
| Analyzer | Standard | Microsystem | ||
|---|---|---|---|---|
| Dead | Total | Dead | Total | |
| II, III | 120 | 3000 | 10 | 500 |
| IV, SX | 120 | 3000 | 30 | 500 |
| V | 90 | 3000 | 10 | 500 |
Storage of Unprocessed Packs: Store at 2-8�C. Do not freeze. Do not expose to temperatures above 35�C or to direct sunlight.
Expiration: Refer to EXPIRATION DATE on the tray label.
Specimen Collection: Serum or urine can be collected and stored by normal procedures. 2
Known Interfering Substances: 3
- Serum Protein Influence. Serum protein levels exert a direct influence on the CREA assay. The following should be taken into account when this method is used for urine samples and when it is calibrated:
Aqueous creatinine standards or urine specimens will give CREA results depressed by approximately 0.7 mg/dL [62 ?mol/L] d and will be less precise than samples containing more than 3 g/dL [30 g/L] protein.
All urine specimens should be diluted with an albumin solution to give a final protein concentration of at least 3 g/dL [30 g/L]. Du Pont Enzyme Diluent (Cat. 790035-901) may be used for this purpose. - High concentration of endrogenous bilirubin (>20 mg/dL [>342 ?mol/L]) will give depressed CREA results (average depression 0.8 mg/dL [71 ?mol/L]). 4
- Grossly hemolyzed (hemoglobin >100 mg/dL [>62 ?mol/L]) or visibly lipemic specimens may cause falsely elevated CREA results. 5,6
- The following cephalosporin antibiotics do not interfere with the CREA method when present at the concentrations indicated. Systematic inaccuracies (bias) due to these substances are less than or equal to 0.1 mg/dL [8.84 ?mol/L] at CREA concentrations of approximately 1 mg/dL [88 ?mol/L].
| Antibiotic | Peak serum level 7,8,9 | Drug concentration | ||
|---|---|---|---|---|
| mg/dL | [mmol/L] | mg/dL | [mmol/L] | |
| Cephaloridine | 1.4 | 0.3 | 25 | 6.0 |
| Cephalexin | 0.6�2.0 | 0.2�0.6 | 25 | 7.2 |
| Cephamandole | 1.3�2.5 | 0.3�0.5 | 25 | 4.9 |
| Cephapirin | 2.0 | D0.4 | 25 | 5.6 |
| Cephradine | 1.5�2.0 | 0.4�0.6 | 25 | 7.1 |
| Cefazolin | 2.5�5.0 | 0.55�1.1 | 50 | 11.0 |
- The following cephalosporin antibiotics have been shown to affect CREA results when present at the indicated concentrations. System inaccuracies (bias) due to these substances are greater than 0.1 mg/dL [8.84 ?mol/L] at CREA concentrations of:
| Antibiotic | Peak serum level 8, 10 | Drug concentration | |||
|---|---|---|---|---|---|
| mg/dL | [mmol/L] | mg/dL | [mmol/L] | Effect | |
| Cephalothin | 1�6 | 0.2�1.5 | 100 | 25.2 | ?20�25% |
| Cephoxitin | 2.0 | 0.5 | 5.0 | 1.2 | ?35�40% |
Systeme International d�unites (S.I. Units) are in brackets.
- The single wavelength measurement used in this method eliminates interference from chromophores whose 510 nm absorbance is constant throughout the measurement period.
- Each laboratory should determine the acceptability of its own blood collection tubes and serum separation products. Variations in these products may exist between manufacturers and, at times, from lot to lot.
Procedure
| Item | II, III, Du Pont Cat. No. | IV, SX, Du Pont Cat. No. | V, Du Pont Cat.No. |
|---|---|---|---|
| ACA� CREA analytical test pack | 701976901 | 701976901 | 701976901 |
| Sample system kit or | 710642901 | 710642901 | 713697901 |
| Micro sample system kit and | 702694901 | 710356901 | NA |
| Micro sample system holders | 702785000 | NA | NA |
| DYLUX� photosensitive | |||
| Printer paper | 700036000 | NA | NA |
| Thermal printer paper | NA | 710639901 | 713645901 |
| Du Pont purified water | 704209901 | 710615901 | 710815901 |
| Cell wash solution | 701864901 | 710664901 | 710864901 |
Test Steps
The operator need only load the sample kit and appropriate test pack(s) into a properly prepared ACA� discrete clinical analyzer. It automatically advances the pack(s) through the test steps and prints a result(s). See the Instrument Manual of the ACA� analyzer for details of mechanical travel of the test pack(s).
Preset Creatinine (CREA) � Test Conditions
- Sample volume: 200 ?L.
- Diluent: purified water.
- Temperature: 37.0 � 0.1�C
- Reaction period: 29 seconds.
- Type of measurement: rate.
- Measurement period: 17.07 seconds.
- Wavelength: 510 nm.
- Units: mg/dL [?mol/L].
Calibration
The general calibration procedure is described in the Calibration/Verification chapter of the Manuals.
The following information should be considered when calibrating the CREA method.
- Assay range: 0-20 mg/mL [0-1768 ?mol/L] e .
- Reference material: Protein containing primary standards f or secondary calibrators such as Du Pont Elevated Chemistry Control (Cat. #790035903) and Normal Chemistry Control (Cat. #790035905) g .
- Suggested calibration levels: 1,5,20, mg/mL, [88, 442, 1768 ?mol/L].
- Calibration scheme: 3 levels, 3 packs per level.
- Frequency: Each new pack lot. Every 3 months for any one pack lot.
| Item | ACA� II analyzer | ACA� III, IV, SX, V analyzer |
|---|---|---|
| Count by | One (1) | NA. |
| [Five (5)] | ||
| Decimal point | 0.0 mg/dL | 000.0 mg/dL |
| Location | [000. ?mol/L] | [000 ?mol/L] |
| Assigned starting | 999.8 | -1.000 E1 |
| Point or offset C 0 | [9823.] | [-8.840 E2] |
| Scale factor or Assigned | 0.2000 mg/dL/count h | 2.004 E-1 h |
| Linear term C 1 h | [0.3536 ?mol/L/count] | [1.772E1] |
Quality Control
Two types of quality control procedures are recommended:
- General instrument check. Refer to the Filter Balance Procedure and the Absorbance Test Method described in the ACA� Analyzer Instrument Manual. Refer also to the ABS Test Methodology literature.
- Creatinine method check. At least once daily run a CREA test on a solution of known creatinine activity such as an assayed control or calibration standard other than that used to calibrate the CREA method. For further details review the Quality Assurance Section of the Chemistry Manual. The result obtained should fall within acceptable limits defined by the day-to-day variability of the system as measured in the user�s laboratory. (See SPECIFIC PERFORMANCE CHARACTERISTICS for guidance.) If the result falls outside the laboratory�s acceptable limits, follow the procedure outlined in the Chemistry Troubleshooting Section of the Chemistry Manual.
A possible system malfunction is indicated when analysis of a sample with five consecutive test packs gives the following results:
| Level | SD |
|---|---|
| 1 mg/dL | >0.15 mg/dL |
| [88 ?mol/L] | [>13 ?mol/L] |
| 20 mg/dL | >0.68 mg/dL |
| [1768 ?mol/L] | [>60 ?mol/L] |
Refer to the procedure outlined in the Trouble Shooting Section of the Manual.
For the results in S.I. units [?mol/L] the conversion factor is 88.4.
Refer to the Creatinine Standard Preparation and Calibration Procedure available on request from a Du Pont Representative.
If the Du Pont Chemistry Controls are being used, prepare them according to the instructions on the product insert sheets.
The preset scale factor (linear term) was derived from the molar absorptivity of the indicator and is based on an absorbance to activity relationship (sensitivity) of 0.596 (mA/min)/(U/L). Due to small differences in filters and electronic components between instruments, the actual scale factor (linear term) may differ slightly from that given above.
Reference interval data obtained from 200 apparently healthy individuals (71 males, 129 females) between the ages of 19 and72.
All Specific Performance Characteristics tests were run after normal recommended equipment quality control checks were performed (see Instrument Manual).
Specimens at each level were analyzed in duplicate for twenty days. The within-run and between-day standard deviations were calculated by the analysis of variance method.
Model equation for regression statistics is: Result of ACA� Analyzer = Slope (Comparative method result) + intercept
See REPRODUCIBILITY for method performance within the assay range.
Results
The ACA� analyzer automatically calculates and prints the CREA result in mg/dL [?mol/L].
Limitation of Procedure
Results > 20 mg/dL [1768 ?mol/L]:
- Dilute with suitable protein base diluent. Reassay. Correct for diluting before reporting.
The reporting system contains error messages to warn the operator of specific malfunctions. Any report slip containing a letter code or word immediately following the numerical value should not be reported. Refer to the Manual for the definition of error codes.
Reference Interval
Serum: 11,i
Males�0.8-1.3 md/dL [71-115 ?mol/L]
Females� 0.6-1.0 md/dL [53-88 ?mol/L]
Urine: 12
Males�0.6-2.5 g/24 hr [53-221 mmol/24 hr]
Females� 0.6-1.5 g/24 hr [53-133 mmol/24 hr]
Each laboratory should establish its own reference intervals for CREA as performed on the analyzer.
Specific Performance Characteristics j
| Material | Mean | Standard deviation (% CV) | |
|---|---|---|---|
| Within-run | Between-day | ||
| Lyophilized | 1.3 | 0.05 (3.7) | 0.05 (3.7) |
| Control | [115] | [4.4] | [4.4] |
| Lyophilized | 20.6 | 0.12 (0.6) | 0.37 (1.8) |
| Control | [1821] | [10.6] | [32.7] |
| Comparative method | Slope | Intercept | Correlation coefficient | n |
|---|---|---|---|---|
| Autoanalyzer� | 1.03 | 0.03[2.7] | 0.997 | 260 |
Assay Range m
0.0�20.0 mg/dl [0-1768 ?mol]
Analytical Specificity
See KNOWN INTERFERING SUBSTANCES section for details.
BIBLIOGRAPHY
1 Larsen, K., Clin Chem Acta 41, 209 (1972).
2 Tietz, NW, Fundamentals of Clinical Chemistry, W. B. Saunders Co., Philadelphia, PA, 1976, pp 47�52, 1211.
3 Supplementary information pertaining to the effects of various drugs and patient conditions on in vivo or in vitro diagnostic levels can be found in �Drug Interferences with Clinical Laboratory Tests,� Clin. Chem 21 (5) (1975), and �Effects of Disease on Clinical Laboratory Tests,� Clin Chem, 26 (4) 1D-476D (1980).
4 Watkins, R. Fieldkamp, SC, Thibert, RJ, and Zak, B, Clin Chem, 21, 1002 (1975).
5 Kawas, EE, Richards, AH, and Bigger, R, An Evaluation of a Kinetic Creatinine Test for the Du Pont ACA, Du Pont Company, Wilmington, DE (February 1973). n
6 Westgard, JO, Effects of Hemolysis and Lipemia on ACA Creatinine Method, 0.200 ?L, Sample Size, Du Pont Company, Wilmington, DE (Oc-tober 972).
7 Physicians� Desk Reference, Medical Economics Company, 33 Edition, 1979.
8 Henry, JB, Clinical Diagnosis and Management by Laboratory Methods, W.B. Saunders Co., Philadelphia, PA 1979, Vol. III.
9 Krupp, MA, Tierney, LM Jr., Jawetz, E, Roe, Rl, Camargo, CA, Physicians Handbook, Lange Medical Publications, Los Altos, CA, 1982 pp 635-636.
10 Sarah, AJ, Koch, TR, Drusano, GL, Celoxitin Falsely Elevates Creatinine Levels, JAMA 247, 205-206 (1982).
11 Gadsden, RH, and Phelps, CA, A Normal Range Study of Amylase in Urine and Serum on the Du Pont ACA, Du Pont Company, Wilmington, DE (March 1978 n ).
12 Dicht, JJ, Reference Intervals for Serum Amylase and Urinary Creatinine on the Du Pont ACA� Discrete Clinical Analyzer, Du Pont Company, Wilmington, DE (November 1984).
Attachment 3 - Analysis of Creatinine for the Normalization of Cadmium and Beta-2-Microglobulin Concentrations in Urine (OSLTC Procedure)
Matrix: Urine
Target Concentration: 1.1 g/L (this amount is representative of creati-nine concentrations found in urine).
Procedure: A 1.0 mL aliquot of urine is passed through a C18 SEP-PAK� (Waters Associates). Approximately 30 mL of HPLC (high performance liquid chromatography) grade water is then run through the SEP-PAK. The resulting solution is diluted to volume in a 100-mL volumetric flask and analyzed by HPLC using an ultraviolet (UV) detector.
Special Requirements: After collection, samples should be appropriately stabilized for cadmium (Cd) analysis by using 10% high purity (with low Cd background levels) nitric acid (exactly 1.0 mL of 10% nitric acid per 10 mL of urine) or stabilized for Beta-2- Microglobulin (B2M) by taking to pH 7 with dilute NaOH (exactly 1.0 mL of 0.11 N NaOH per 10 mL of urine). If not immediately analyzed, the samples should be frozen and shipped by overnight mail in an insulated container.
Dated: January 1992.
Chemists: David B. Armitage, Duane Lee,
Organic Service Branch II, OSHA Technical Center, Salt Lake City, Utah.
1. General Discussion
1.1. Background
1.1.1. History of procedure
Creatinine has been analyzed by several methods in the past. The earliest methods were of the wet chemical type. As an example, creatinine reacts with sodium picrate in basic solution to form a red complex, which is then analyzed colorimetrically (Refs. 5.1. and 5.2.).
Since industrial hygiene laboratories will be analyzing for Cd and B2M in urine, they will be normalizing those concentrations to the concentration of creatinine in urine. A literature search revealed several HPLC methods (Refs. 5.3., 5.4., 5.5. and 5.6.) for creatinine in urine and because many industrial hygiene laboratories have HPLC equipment, it was desirable to develop an industrial hygiene HPLC method for creatinine in urine. The method of Hausen, Fuchs, and Wachter was chosen as the starting point for method development. SEP-PAKs were used for sample clarification and cleanup in this method to protect the analytical column. The urine aliquot which has been passed through the SEP-PAK is then analyzed by reverse-phase HPLC using ion-pair techniques.
This method is very similar to that of Ogata and Taguchi (Ref. 5.6.), except they used centrifugation for sample clean-up. It is also of note that they did a comparison of their HPLC results to those of the Jaffe method (a picric acid method commonly used in the health care industry) and found a linear relationship of close to 1:1. This indicates that either HPLC or colorimetric methods may be used to measure creatinine concentrations in urine.
1.1.2. Physical properties (Ref. 5.7.)
Molecular weight: 113.12
Molecular formula: C 4 -H 7 -N 3 -O
Chemical name: 2-amino-1,5-dihydro-1-methyl-4H-imidazol-4-one
CAS: 60-27-5
Melting point: 300�C (decomposes)
Appearance: white powder
Solubility: soluble in water; slightly soluble in alcohol; practically insoluble in acetone, ether, and chloroform
Synonyms: 1-methylglycocyamidine, 1-methylhydantion-2-imide
Structure: see Figure 1 
1.2 Advantages
1.2.1. This method offers a simple, straightforward, and specific alternative method to the Jaffe method.
1.2.2. HPLC instrumentation is commonly found in many industrial hygiene laboratories.
2. Sample Stabilization Procedure
2.1. Apparatus
Metal-free plastic container for urine sample.
2.2. Reagents
2.2.1. Stabilizing Solution�1) Nitric acid (10%, high purity with low Cd background levels) for stabilizing urine for Cd analysis or 2) NaOH, 0.11 N, for stabilizing urine for B2M analysis.
2.2.2. HPLC grade water
2.3. Technique
2.3.1. Stabilizing solution is added to the urine sample (see section 2.2.1.). The stabilizing solution should be such that for each 10 mL of urine, add exactly 1.0 mL of stabilizer solution. (Never add water or urine to acid or base. Always add acid or base to water or urine.) Exactly 1.0 mL of 0.11 N NaOH added to 10 mL of urine should result in a pH of 7. Or add 1.0 mL of 10% nitric acid to 10 mL of urine.
2.3.2. After sample collection seal the plastic bottle securely and wrap it with an appropriate seal. Urine samples should be frozen and then shipped by overnight mail (if shipping is necessary) in an insulated container. (Do not fill plastic bottle too full. This will allow for expansion of contents during the freezing process.)
2.4. The Effect of Preparation and Stabilization Techniques on Creatinine Concentrations
Three urine samples were prepared by making one sample acidic, not treating a second sample, and adjusting a third sample to pH 7. The samples were analyzed in duplicate by two different procedures. For the first procedure a 1.0 mL aliquot of urine was put in a 100-mL volumetric flask, diluted to volume with HPLC grade water, and then analyzed directly on an HPLC. The other procedure used SEP-PAKs. The SEP-PAK was rinsed with approximately 5 mL of methanol followed by approximately 10 mL of HPLC grade water and both rinses were discarded. Then, 1.0 mL of the urine sample was put through the SEP-PAK, followed by 30 mL of HPLC grade water. The urine and water were transferred to a 100-mL volumetric flask, diluted to volume with HPLC grade water, and analyzed by HPLC. These three urine samples were analyzed on the day they were obtained and then frozen. The results show that whether the urine is acidic, untreated or adjusted to pH 7, the resulting answer for creatinine is essentially unchanged. The purpose of stabilizing the urine by making it acidic or neutral is for the analysis of Cd or B2M respectively.
| Sample | w/o SEP-PAK(g/L creatinine) | with SEP-PAK(g/L creatinine) |
|---|---|---|
| Acid | 1.10 | 1.10 |
| Acid | 1.11 | 1.10 |
| Untreated | 1.12 | 1.11 |
| Untreated | 1.11 | 1.12 |
| pH7 | 1.08 | 1.02 |
| pH7 | 1.11 | 1.08 |
2.5. Storage
After 4 days and 54 days of storage in a freezer, the samples were thawed, brought to room temperature and analyzed using the same procedures as in section 2.4. The results of several days of storage show that the resulting answer for creatinine is essentially unchanged.
| 4 days | 54 days | |||
|---|---|---|---|---|
| Sample | w/o SEPPAK (g/L creatinine) | with SEPPAK (g/L creatinine) | w/o SEPPAK (g/L creatinine) | with SEPPAK (g/L creatinine) |
| Acid | 1.09 | 1.09 | 1.08 | 1.09 |
| Acid | 1.10 | 1.10 | 1.09 | 1.10 |
| Acid | 1.09 | 1.09 | ||
| Untreated. | 1.13 | 1.14 | 1.09 | 1.11 |
| Untreated. | 1.15 | 1.14 | 1.10 | 1.10 |
| Untreated. | 1.09 | 1.10 | ||
| pH 7 | 1.14 | 1.13 | 1.12 | 1.12 |
| pH 7 | 1.14 | 1.13 | 1.12 | 1.12 |
| pH 7 | 1.12 | 1.12 | ||
2.6. lnterferences � None.
2.7. Safety precautions
2.7.1. Make sure samples are properly sealed and frozen before shipment to avoid leakage.
2.7.2. Follow the appropriate shipping procedures.
The following modified special safety precautions are based on those recommended by the Centers for Disease Control (CDC)(Ref. 5.8.) and OSHA�s Bloodborne Pathogens standard (29 CFR 1910.1030).
2.7.3. Wear gloves, lab coat, and safety glasses while handling all human urine products. Disposable plastic, glass, and paper (pipet tips, gloves, etc.) that contact urine should be placed in a biohazard autoclave bag. These bags should be kept in appropriate containers until sealed and autoclaved. Wipe down all work surfaces with 10% sodium hypochlorite solution when work is finished.
2.7.4. Dispose of all biological samples and diluted specimens in a biohazard autoclave bag at the end of the analytical run.
2.7.5. Special care should be taken when handling and dispensing nitric acid. Always remember to add acid to water (or urine). Nitric acid is a corrosive chemical capable of severe eye and skin damage. Wear metal-free gloves, a lab coat, and safety glasses. If the nitric acid comes in contact with any part of the body, quickly wash with copious quantities of water for at least 15 minutes.
2.7.6. Special care should be taken when handling and dispensing NaOH. Always remember to add base to water (or urine). NaOH can cause severe eye and skin damage. Always wear the appropriate gloves, a lab coat, and safety glasses. If the NaOH comes in contact with any part of the body, quickly wash with copious quantities of water for at least 15 minutes.
3. Analytical Procedure
3.1. Apparatus
3.1.1. A high performance liquid chromatograph equipped with pump, sample injector and UV detector.
3.1.2. A C18 HPLC column; 25 cm x 4.6 mm I.D.
3.1.3. An electronic integrator, or some other suitable means of determining analyte response.
3.1.4. Stripchart recorder.
3.1.5. C18 SEP-PAKs (Waters Associates) or equivalent.
3.1.6. Luer-lock syringe for sample preparation (5 mL or 10 mL).
3.1.7. Volumetric pipettes and flasks for standard and sample preparation.
3.1.8. Vacuum system to aid sample preparation (optional).
3.2. Reagents
3.2.1. Water, HPLC grade.
3.2.2. Methanol, HPLC grade.
3.2.3. PlC B-7� (Waters Associates) in small vials.
3.2.4. Creatinine, anhydrous, Sigma Chemical Corp., purity not listed.
3.2.5. 1-Heptanesulfonic acid, sodium salt monohydrate.
3.2.6. Phosphoric acid.
3.2.7. Mobile phase. It can be prepared by mixing one vial of PlC B-7 into a 1 L solution of 50% methanol and 50% water. The mobile phase can also be made by preparing a solution that is 50% methanol and 50% water with 0.005M heptanesulfonic acid and adjusting the pH of the solution to 3.5 with phosphoric acid.
3.3. Standard preparation
3.3.1. Stock standards are prepared by weighing 10 to 1 mg of creatinine. This is transferred to a 25-mL volumetric flask and diluted to volume with HPLC grade water.
3.3.2. Dilutions to a working range of 3 to 35 ?g/mL are made in either HPLC grade water or HPLC mobile phase (standards give the same detector response in either solution).
3.4. Sample preparation
3.4.1. The C18 SEP-PAK is connected to a Luer-lock syringe. It is rinsed with 5 mL HPLC grade methanol and then 10 mL of HPLC grade water. These rinses are discarded.
3.4.2. Exactly 1.0 mL of urine is pipetted into the syringe. The urine is put through the SEP-PAK into a suitable container using a vacuum system.
3.4.3. The walls of the syringe are rinsed in several stages with a total of approximately 30 mL of HPLC grade water. These rinses are put through the SEP-PAK into the same container. The resulting solution is transferred to a 100-mL volumetric flask and then brought to volume with HPLC grade water.
3.5. Analysis (conditions and hardware are those used in this evaluation.)
3.5.1. Instrument conditions
| Column | Zorbax� ODS, 5-6 ?m particle size; 25 cm X 4.6 mm I.D. |
| Mobile phase | See Section 3.2.7. |
| Detector | Dual wavelength UV; 229 nm (primary) 254 nm (secondary), |
| Flow rate | 0.7 mL/minute. |
| Retention time | 7.2 minutes. |
| Sensitivity | 0.05 AUFS. |
| Injection volume | 20 ?L. |
3.5.2. Chromatogram (See Figure #2).
3.6. Interferences
3.6.1. Any compound that has the same retention time as creatinine and absorbs at 229 nm is an interference.
3.6.2. HPLC conditions may be varied to circumvent interferences. In addition, analysis at another UV wavelength (i.e. 254 nm) would allow a comparison of the ratio of response of a standard to that of a sample. Any deviations would indicate an interference.
3.7. Calculations
3.7.1. A calibration curve is constructed by plotting detector response versus standard concentration (See Figure #3).
3.7.2. The concentration of creatinine in a sample is determined by finding the concentration corresponding to its detector response. (See Figure #3).
3.7.3. The ?g/mL creatinine from section 3.7.2. is then multiplied by 100 (the dilution factor). This value is equivalent to the micrograms of creatinine in the 1.0 mL stabilized urine aliquot or the milligrams of creatinine per liter of urine. The desired unit, g/L, is determined by the following relationship:
 |
3.7.4. The resulting value for creatinine is used to normalize the urinary concentration of the desired analyte (A) (Cd or B2M) by using the following formula.
 |
Where A is the desired analyte. The protocol of reporting such normalized results is ?g A/g creatinine.
3.8. Safety precautions. See section 2.7.
4. Conclusions
The determination of creatinine in urine by HPLC is a good alternative to the Jaffe method for industrial hygiene laboratories. Sample clarification with SEP-PAKs did not change the amount of creatinine found in urine samples. However, it does protect the analytical column. The results of this creatinine in urine procedure are unaffected by the pH of the urine sample under the conditions tested by this procedure. Therefore, no special measures are required for creatinine analysis whether the urine sample has been stabilized with 10% nitric acid for the Cd analysis or brought to a pH of 7 with 0.11 NaOH for the B2M analysis.
5. References
5.1. Clark, L.C.; Thompson, H.L.; Anal. Chem. 1949, 21, 1218.
5.2. Peters, J.H.; J. Biol. Chem. 1942, 146, 176.
5.3. Hausen, V.A.; Fuchs, D.; Wachter, H.; J. Clin. Chem. Clin. Biochem. 1981, 19, 373-378.
5.4. Clark, P.M.S.; Kricka, L.J.; Patel, A.; J. Liq. Chrom. 1980, 3(7), 1031-1046.
5.5. Ballerini, R.; Chinol, M.; Cambi, A.; J. Chrom. 1979, 179, 365-369.
5.6. Ogata, M.; Taguchi, T.; Industrial Health 1987, 25, 225�228.
5.7. �Merck Index�, 11th ed.; Windholz, Martha Ed.; Merck: Rahway, N.J., 1989; p. 403.
5.8. Kimberly, M.; � Determination of Cadmium in Urine by Graphite Furnace Atomic Absorption Spectrometry with Zeeman Background Correction. � Centers for Disease Control, Atlanta, Georgia, unpublished, update 1990.
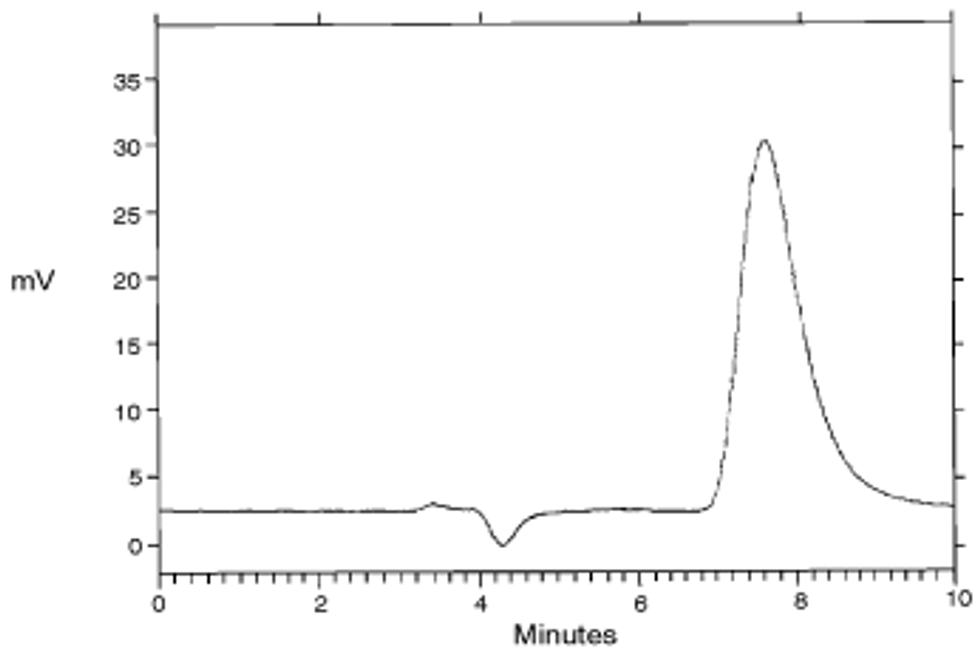 |
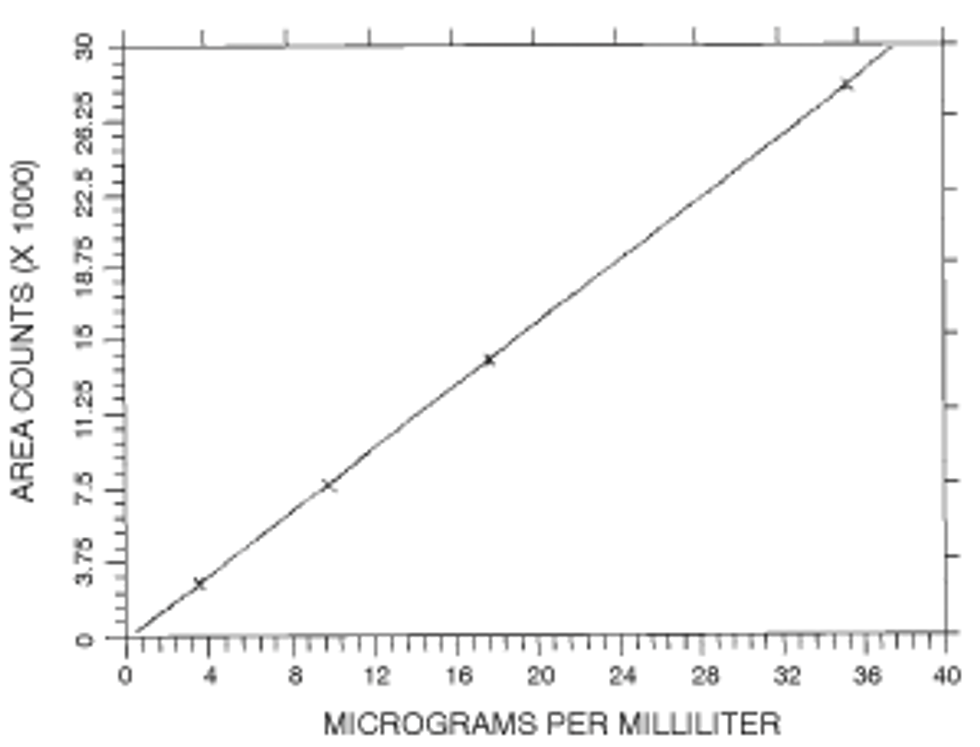 |
['Toxic and Hazardous Substances - OSHA']
['Toxic and Hazardous Substances - OSHA', 'Cadmium']
UPGRADE TO CONTINUE READING